

Murata et al Confirm My Spike Protein Heart Failure Hypothesis
And the mechanism is ischemia-reperfusion injury - precisely the one I identified.

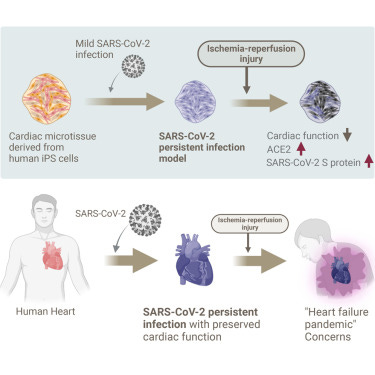
In October of last year, I wrote a post hypothesizing how I believed the Spike Protein was causing heart failure by inducing “silent heart attacks.” The result of these “silent heart attacks” (microvascular injury by the Spike Protein) would result in heart failure. The mechanism I proposed was that this damage was not a one-time event. It would be persistent due to repeated (or persistent) exposure to the Spike Protein.
It is very clear that the microvascular damage caused by the Spike Protein’s attack on the endothelium, in essence, replicates a “mild” heart attack. By virtue of its effect on the microvasculature, it also induces “liver attacks,” “brain attacks,” “kidney attacks” and so forth via the same mechanism. Also, the post-myocardial infarction damage of ischemia-reperfusion injury, additionally, occurs.
THE SPIKE PROTEIN’S EFFECT ON THE MICROVASCULATURE OF THE HEART AND OTHER ORGANS IS EQUIVALENT TO A SILENT “HEART ATTACK.” ADDITIONAL DAMAGE FROM ISCHEMIA-REPERFUSION INJURY
https://wmcresearch.substack.com/p/the-spike-proteins-effect-on-the
On December 22nd of this year, a paper was published which, through the use of human iPS cell-derived cardiac microtissues, proved my hypothesis to be correct, and via the mechanism I identified.
Accordingly, co-localization of cTnT and S protein was facilitated by the hypoxia, indicating intracellular reactivation of SARS-CoV-2 (Figure 2D). Nevertheless, the viral titer was not increased by the hypoxia which may imply the manner of the reactivation of SARS-CoV-2 which would not increase infectivity to other tissue but boost intracellular activity of SARS-CoV-2 (Figure S2). IFA for CD31 revealed that vascular network formation was globally fragmented in persistent infection model with SARS-CoV-2 after ischemia and reperfusion, whereas it was maintained in MOCK (Figure 2E). These results indicate that the hypoxic stress disrupted vascular network formation possibly because of the reactivation of SARS-CoV-2 and conferred functional deterioration of the infected CMTs.
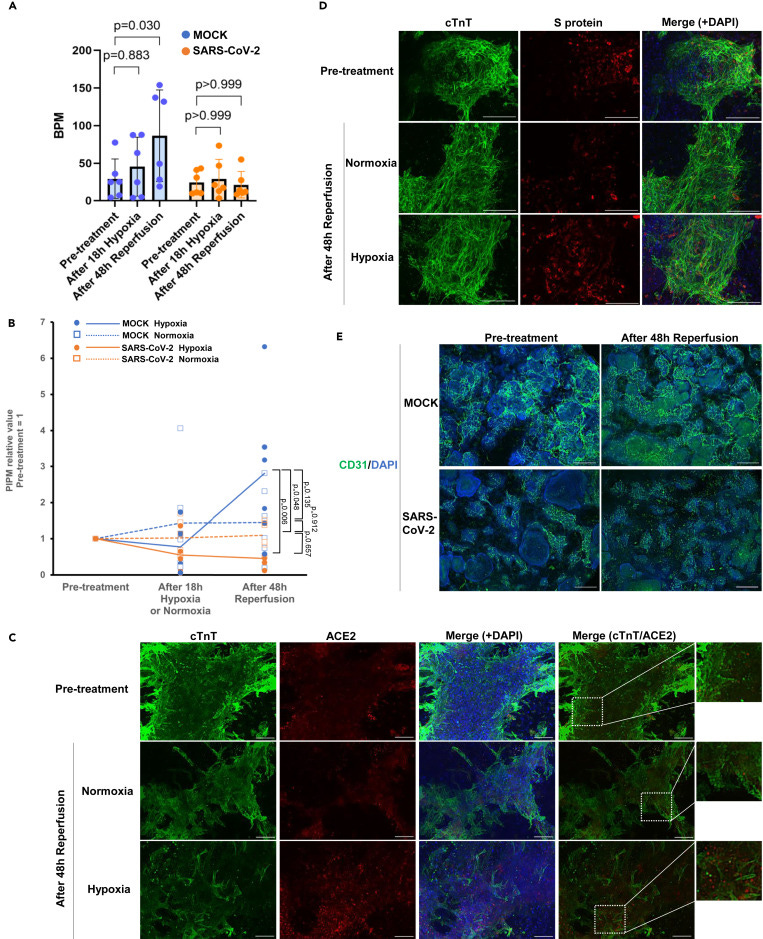
Figure 2 Deterioration of the tissue function of persistent infection model of SARS-CoV-2 triggered by hypoxic stress
(A and B) Assessment of cardiac function. “SARS-CoV-2” indicates persistent infection model of SARS-CoV-2. (A) Beats per minute (BPM) at pre-treatment and after 48h of reperfusion condition (n = 6 each). Error bars show S.D. B, PIPM over time (n = 6 each).
(C and D) IFA for persistent infection model of SARS-CoV-2 before treatment (Pre-treatment), 18h of hypoxia treatment (Hypoxia) or Normoxia followed by 48h reperfusion treatment. (C) cTnT (Green) and ACE2 (Red). (D) cTnT (Green) and S protein (Red). (E) CD31 (Green). Scale bars: C,D,100 μm. (E) 500 μm. Nuclei were stained with DAPI (Blue).
I also predicted that this would cause a tsunami of incoming cardiac issues.
Spike Protein Induced Cardiotoxicity: A Potential Tsunami of Cardiac Issues Over the Next 20+ Years
https://wmcresearch.substack.com/p/spike-protein-induced-cardiotoxicity
Murata, et al also came to the same conclusion.
In conclusion, this report may serve as a warning for the possibility of a heart failure pandemic in the post COVID-19 era. As a countermeasure against this global healthcare risk, this model would serve as a useful tool to investigate the mechanism of the onset and the progression of SARS-CoV-2 cardiomyopathy and to develop therapeutic options.
Predicted risk of heart failure pandemic due to persistent SARS-CoV-2 infection using a three-dimensional cardiac model
https://www.cell.com/iscience/fulltext/S2589-0042(23)02718-9
Though this news is not what we were hoping for, I am increasingly convinced that a plan to remove the Spike Protein and repair/regenerate the affected tissues may ameliorate the injury and disease this unnatural (in my opinion) pathogen causes, destroying our cells.
I will continue to work. We must move forward with hope and understanding. Please have a Happy New Year and, as always, thank you for your readership and support!
I would like to understand more facts so as to distinguish between injury from SARS-CoV-2 infection and injury from mRNA injection. How many Spike protein subunits are produced in a typical infection vs. an mRNA injection? What are the measures of central tendency for that data, i.e. mean, median and mode?
What systems / organs are typically affected by a SARS-Cov-2 infection? I mean a "typical" case. I suspect the typical infection is localized to upper and lower respiratory tracts in most cases, with digestive tract coming second. I suspect most other organ systems are spared, meaning that a typical infection does not necessarily introduce Spike to the endothelial layer of our circulatory systems. To put an ironic point on it, in contrast, I suspect that the typical mRNA injection sends spike to all organs (with preference to the reproductive organs, spleen and pancreas, with other organs not far behind) (i.e. the heart). Of course that's where pharma and government lied to us about the mRNA staying "localized," which was disproven by the Japan biodistribution study results in rodents.
Obviously much of this information will never be learned. But the "count" of Spike protein subunits for typical infection vs. mRNA injection should be a number we know. Does anyone have a link to a coherent estimate?
*edit* - Here's Karl Denninger addressing some of the same topic a day later:
https://market-ticker.org/akcs-www?post=250384
There is a world of difference to catching Covid via nasal and lung pathways.. which any healthy immune system should be able to control and eradicate.. to introducing a huge carrier load straight into the blood stream and over whelming the immune system(Trojan horses) what science thinks it’s a clever idea to create something that has no off switch... and possibly reverse transcribe into the DNA and manufacture spike proteins for months after months?... the immune system banks reserves will soon deplete... buffoons disguised as boffins got us into this mess... so now we need to avoid anyone wearing a white coat brandishing the needle of death.