


A CEREBROGENIC HYPOTHESIS FOR THE OBSERVED NON-MYOCARDITIS SUDDEN CARDIAC DEATHS
The Spike Protein damaging the brainstem inducing fatal arrhythmia

It has been documented that the Spike Protein is responsible for direct inflammation of the heart, resulting in myocarditis and sudden death.
We present autopsy findings of a 22-year-old man who developed chest pain 5 days after the first dose of the BNT162b2 mRNA vaccine and died 7 hours later. Histological examination of the heart revealed isolated atrial myocarditis, with neutrophil and histiocyte predominance. Immunohistochemical C4d staining revealed scattered single-cell necrosis of myocytes which was not accompanied by inflammatory infiltrates. Extensive contraction band necrosis was observed in the atria and ventricles. There was no evidence of microthrombosis or infection in the heart and other organs. The primary cause of death was determined to be myocarditis, causally-associated with the BNT162b2 vaccine.
Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8524235/
However, there have been a plethora of recent sudden cardiac deaths observed very likely long after vaccination and/or infection with SARS-CoV-2. This disturbing trend has finally made the main stream media.
The number of deaths registered in England and Wales due to cardiac arrhythmias was more than usual for much of the first half of 2022, according to the Office for National Statistics (ONS).
Deaths in this category had the second highest excess mortality figures in March and April, up from being the eighth highest in February and the fourth highest in January.
More people have been dying this year due to irregular heartbeat, official figures suggest
https://news.sky.com/story/irregular-heartbeat-likely-to-be-one-of-the-reasons-more-people-than-usual-have-been-dying-this-year-12701948
As most of these sudden cardiac deaths have revealed no heart disease upon autopsy (from what I have read), we are left looking for another mechanism. I believe a very strong candidate for explaining these fatalities is lesions of the brainstem, caused by the Spike Protein.
Let us look at the evidence supporting this hypothesis.
The Spike Protein has been found in the brainstem of autopsied patients.
Whole brain from 43 patients (27 males and 16 females; 51–94 years; Hamburg, Germany).
Pronounced inflammation (leukocyte infiltration and microglial and astrocytic activations) in most cases that were most evident in the cerebellum and medulla.
Positive SARS-CoV-2 RNA in the frontal lobe (9 out of 23 patients) and brainstem (4 out of 8 patients).
Positive SARS-CoV-2 nucleocapsid or spike protein in the medulla and its neural connections (glossopharyngeal or vagal cranial nerves) in 16 out of 40 patients.
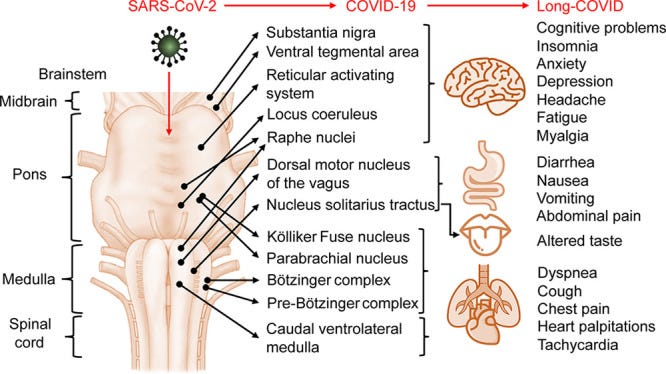
Indeed, the symptoms of Long COVID overlap with brainstem dysfunction.
Others have also raised the idea of SARS-CoV-2 tropism for the brainstem as a possible cause of respiratory failure in COVID-19. This is because the brain’s cardiorespiratory center is located in the brainstem. However, the brainstem consisting of the medulla, pons, and midbrain also plays other roles besides respiratory regulation, such as maintaining cardiovascular, gastrointestinal, and neurological processes. Since both peripheral and central neuronal injury may be permanent and regeneration is extremely rare and slow, brainstem injury may be long-lasting as well. Interestingly, functions of the brainstem and symptoms of long-COVID overlap to a great extent.
Persistent Brainstem Dysfunction in Long-COVID: A Hypothesis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7874499/
Direct invasion is not the only way Spike Protein can damage the brainstem. SPED is also a cause of brainstem injury.
A 66-year-old man, diabetic, hypertensive, admitted to the emergency room for medical management of acute dyspnea, diagnosed with COVID-19 infection. The evolution is marked by respiratory distress as well as new onset atrial fibrillation and a severe ischemic stroke of the brainstem. COVID-19 disease is associated with very serious thromboembolic complications of high incidence, and this is explained by the coagulopathy secondary to the alteration of the microcirculation after the hyper-inflammatory state.
Brainstem stroke: A fatal thromboembolic event after new onset atrial fibrillation during covid-19 infection: A case report and literature review
https://www.sciencedirect.com/science/article/pii/S1930043321005653
Additionally, Molecular Mimicry (I believe most likely by the Spike Protein, due to its massive epitope sharing with human proteins) appears to be creating AUTOANTIBODIES AGAINST THE BRAINSTEM!
The newly discovered anti-neuronal antibodies might be promising markers of severe disease and the targeted peptide epitopes might be used for targeted immunomodulation. Further work is needed to determine whether these antibodies may play a role in long-COVID.
Anti-neuronal antibodies against brainstem antigens are associated with COVID-19
https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(22)00393-0/fulltext
So, what is the point? The point is that IF THE BRAINSTEM IS BEING PROGESSIVELY AND CONSTANTLY ATTACKED, EVENTUALLY THE DAMAGE WILL TRIGGER A FATAL ARRHYTHMIA.
I believe the Spike Protein is injuring the brainstem in precisely the same way as a stroke. In fact, in some cases, the damage may be from a thromboembolic event.
A 52-year-old man presented with vomiting, dysphagia, left-sided ataxia and dissociated sensory loss. Diffusion-weighted MRI showed evidence of acute infarct in the left lateral medulla and left medial cerebellar hemisphere, probably secondary to thromboembolism from left vertebral artery dissection. While making an uneventful recovery as an inpatient, a routine 24 h ECG was performed 2 weeks after the stroke to investigate possible paroxysmal atrial fibrillation. The recording instead revealed 56 asymptomatic episodes of sinus arrest, necessitating implantation of a permanent pacemaker to prevent sudden cardiac death. The medulla contains key structures involved in autonomic regulation, including the dorsal vagal nucleus and the nucleus tractus solitarius.
An unexpected Holter monitor result: multiple sinus arrests in a patient with lateral medullary syndrome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3604361/
I believe, like this individual, those who are dying from sudden cardiac arrest due to this mechanism, may be experiencing symptoms of cardiac arrest, perhaps many, many times before the fatal event, yet because they are young and seemingly full of health, they dismiss the warning signs as fatigue or stress.
As many of those who have followed my work know, I believe this is yet another example of how SARS-CoV-2 and its Spike Protein create a pathologic “whack-a-mole” environment. If it’s not thromboembolism that damages the brainstem, it’s the autoantibodies, etc.
I do not believe we should be resting easy that the acute symptoms of COVID-19 appear to be easing. I once again ask all readers to consider China’s continued zero COVID stance. Could it be they know information we are just gleaning? For example, does the Spike Protein inexorably march to the brainstem? To cause a sudden, fast and “merciful execution?”
I apologize for waxing morbid, but I am extremely concerned. After all. It wouldn’t be the first-time viral proteins have traveled to the brain to cause certain death. I will sum this concern up with just one word: Rabies.
Let’s hope we find a therapeutic to degrade the Spike Protein, and if it is replicating, ways to inhibit this. Could we be dealing with another HIV-like lurker?
I will continue to work on the mechanisms of the Spike Protein and on therapeutics to combat it.
I am extremely grateful to all supporters, and a special thank you to those who can financially contribute towards my work. I spend most of my time reading and researching this disease. Once we have it fully understood and treated, I will return to working on Obesity.











Just read an article on Dr. Ralph Baric UNC Chapel Hill. Clear back in the 80’s he was studying this EXACT topic, and not for good reasons, it looks. All paid for by the defense department and usual suspects.
Thank you Walter.