

The Spike Protein, Baroreceptors and Sudden Death: Think Pilots
The Spike Protein’s presence in Baroreceptor locations may fatally disrupt communication between the brain and the heart.

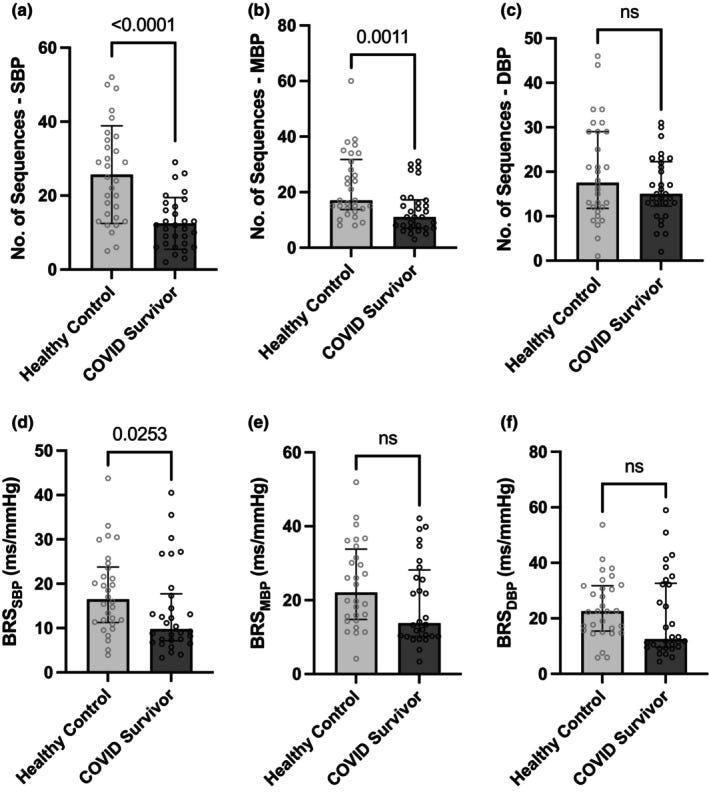
Comparison of the time domain measures of BRS computed by the spontaneous sequence between the COVID survivor and matched healthy control group. (a–c) represents the number of sequences and (d–f) the BRS quantified, respectively, for SBP‐, MBP‐, and DBP‐based analysis. (BRS, baroreflex sensitivity; DBP, diastolic blood pressure; MBP, mean blood pressure; SBP, systolic blood pressure). Error bars represent standard deviation in (a) and 25th centile–75th centile in (b–f). Unpaired t test is used for the statistical comparison between the two groups in (a); Mann–Whitney test is used in (b–f).
This is a very important post. One which I hope other researchers and clinicians will use to spur additional research and therapeutic pursuits.
I present here an additional mechanism by which the Spike Protein may be causing the astronomically elevated number of sudden cardiac deaths being observed worldwide. This mechanism is the impairment of the body’s Baroreceptors by the Spike Protein.
It was noted early in the pandemic that the interaction of the Spike Protein with ACE2 was causing problems with the carotid bodies. Recall the “happy hypoxics.”
Herein, we have focused on the carotid bodies. In this hypothetical viewpoint, we have discussed the plasticity of the carotid body chemoreflex and made a comparison between acute and chronic exposures to high altitude with COVID-19. From these discussions, we have postulated that the sensitivity of the hypoxic ventilatory response may well determine the outcome of disease severity and those that live at high altitude may be more resistant. We have provided insight into silent hypoxia and attempted to explain an absence of ventilatory drive and anxiety yet maintenance of consciousness.
Relevance of carotid bodies in COVID-19: A hypothetical viewpoint
https://pmc.ncbi.nlm.nih.gov/articles/PMC8052558/
And, yet, there are Baroreceptors located in the immediately adjacent carotid sinuses.
There are two types of baroreceptors:
High-pressure arterial baroreceptors and low-pressure volume receptors which are both stimulated by stretching of the vessel wall. Arterial baroreceptors are located within the carotid sinuses and the aortic arch.
Low-pressure volume receptors, or cardiopulmonary receptors, are located within the atria, ventricles, and pulmonary vasculature.
Baroreceptors
https://www.physio-pedia.com/Baroreceptors
Indeed, it has been shown that due to the Spike Protein’s binding to ACE2, this damages the baroreceptors and their ability to communicate with the brainstem.
Possible damages to the afferent hypoxia-sensing neuros could be due to the direct effect of COVID-19 by binding ACE2 expressed in capillary endothelium of BBB to gain access into the CNS28 or by indirect effect with cytokine storm on mitochondria or on nerve fibers29. Recent PET (positron emission tomography) scan findings have highlighted that COVID-19 neurotropism could occur in patients with impairment of olfactory bulb but also in other limbic structures, including thalamus/hypothalamus, cerebellum and the brainstem.
Impairs of the HRV (heart rate variability) may be explained by the acute dysautonomia enhancing by afferent baroreflex failure. This mechanism leads to several damages at the afferent baroreceptor signaling, which starts from baroreceptors in carotid bodies to the vagal and glossopharyngeal nerve fibers, and then, to the NTS.
Clinical characterization of dysautonomia in long COVID-19 patients
https://www.nature.com/articles/s41598-021-93546-5
This is an absolutely convincing explanation as to why we are observing a surge in sudden cardiac deaths – especially among pilots.
Baroreflex, a cardiovascular response, will be fully activated to restore blood pressure and to enhance G tolerance when aircrews are subjected to sustained G stress. The average of relaxed G tolerance (RGT) is from 4.5 to 6G, determined at a gradual onset rate (GOR) run. The protective mechanism is modulated by sympathetic vasoconstriction and parasympathetic heart rate (HR) increase. HR increase could be an indicator of baroreflex activation to compensate for the drop of cerebral blood perfusion during the G exposure6–8. Compared with the low-G tolerance group, there were higher HR responses in the high-G tolerance group under a mild hypergravity environment.
Combined effect of heart rate responses and the anti-G straining manoeuvre effectiveness on G tolerance in a human centrifuge
https://pmc.ncbi.nlm.nih.gov/articles/PMC7730161/
And yet, we will hear the eternal chorus of Spike Deniers singing “Why is this not happening to everyone, then?” The Spike Protein is diabolical. It is not a guillotine for nine billion heads. It is a conveyor belt for nine billion heads with a guillotine at the end of it.
And the answer is simple: everyone has a unique baroreflex sensitivity.
We have suggested that among conscious dogs with a healed anterior wall myocardial infarction (MI) a depressed baroreflex sensitivity (BRS) carries a higher risk of developing ventricular fibrillation during a brief ischemic episode associated with an exercise stress test.
Autonomic Mechanisms and Sudden Death
https://www.ahajournals.org/doi/epdf/10.1161/01.CIR.78.4.969
An additional observation: Why are the depressed more likely to experience more severe/fatal Spike/SARS-CoV-2 issues?
Results: BRS was significantly lower in patients than in controls (19.5 [1.78] versus 25.4 [1.69] ms/mm Hg, p = .017). Analysis of covariance, in which age, sex, cholesterol, and body mass index were included, also showed that depression was a significant (p = .027) predictor of BRS. There was no significant difference in BRS adjusted by age and sex between the subjects taking antidepressants compared with those on no medications (p = .40).
Conclusions: These data indicate that BRS is impaired in otherwise healthy patients with depression and may contribute to their increased cardiac risk.
Baroreflex sensitivity is reduced in depression
https://pubmed.ncbi.nlm.nih.gov/16046382/
Again, we must ask ourselves: Is this slowly, inexorably occurring in each of us, with each exposure to SARS-CoV-2 and its Spike Protein? Is our own BRS being gradually impaired? We must continue to search for and find answers. God bless the Pilots, and the rest of us.
Thank you, as always, for your continued support, dialog and readership. I will continue to work and to find ways to ameliorate the damages which are being inflicted upon mankind.
I have to agree with this data. I began my first episode of adverse cardiac events 2 weeks after the Moderna vaccine- I was at 12000 feet skiing (Breckenridge) when I had issues with ventricular arrhythmias- continue to have it. I have POTS syndrome now. I was hospitalized with Takotsubo Cardiomyopathy June 2022 which I absolutely feel was related to the vaccine and exposure to COVID. I was otherwise healthy running marathons until I rec'd 1 moderna vaccination!!! I have been an athlete my whole life and never had these issues prior to the vaccine. I should point out I was skiing 4 weeks prior to the onset of the ventricular arrhythmias in Park City and had absolutely no issues. It only began after Moderna vaccine.
The other reason for the difference in response to spike protein or the individual effects caused by the shots is due to Batch or Lot variance. In one case where Germany looked at the Lot data from Denmark it was noted that the quality varied significantly between Lot batches such that some vials would have little to any of the specified substances and others were way over the recommended or spec levels. This has been noted and written about in nearly all countries who were vaccinating their citizens. Japan had to remove around 140,000 vials of COVID vaccine due to “ excessive magnetic properties “.