

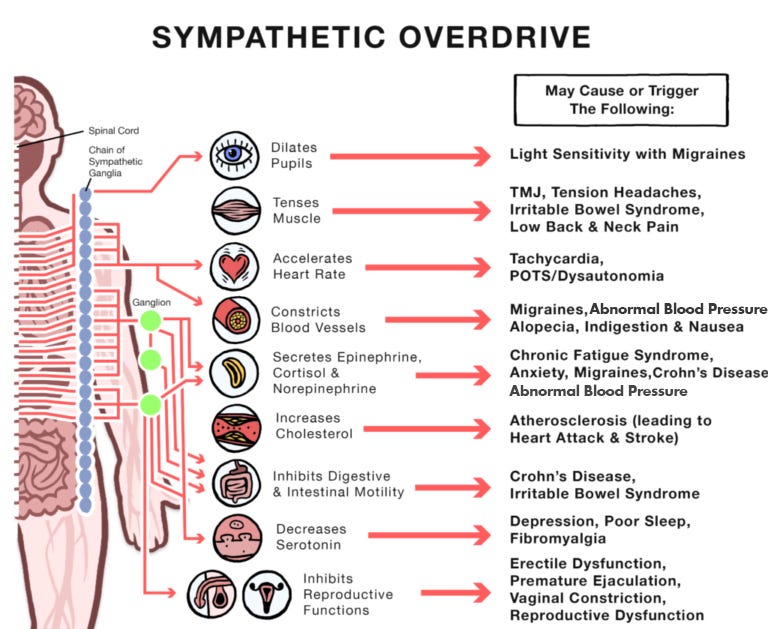
THE AMYGDALA, SYMPATHETIC OVERDRIVE AND ELEVATED CATECHOLAMINE LEVELS: THE SPIKE PROTEIN’S INDUCTION OF LONG COVID AS A CONSTANT STATE OF “FEAR OR FLIGHT” RESPONSE
The relevance of Takotsubo Syndrome; Spike Protein Sudden Cardiac Death due to 1) Cardiac Invasion 2) Neuroinvasion

It is known that the Spike Protein is inducing Myocarditis and is responsible for an increasing number of Sudden Cardiac Deaths, particularly in young and previously healthy individuals. However, I have been concerned about the number of sudden deaths which are occurring in those who had not recently been exposed to the Spike Protein. Continuing my recent research into the Spike Protein’s ability to invade the brainstem. I have found a mechanism by which cerebral damage can cause the same Takotsubo Syndrome associated with COVID mRNA vaccination.
Takutsubo Cardiomyopathy has been observed following COVID-19 vaccination.
Concerns have been raised recently about takotsubo cardiomyopathy (TCM) after receiving COVID-19 vaccines, particularly the messenger RNA (mRNA) vaccines. The goal of this study was to compile case reports to provide a comprehensive overview of takotsubo cardiomyopathy (TCM) associated with COVID-19 vaccines. A systematic literature search was conducted in PubMed, Scopus, Embase, Web of Science, and Google Scholar between 2020 and June 1, 2022. The study included individuals who developed cardiac takotsubo cardiomyopathy from receiving COVID-19 vaccinations. Ten studies, including 10 cases, participated in the current systematic review. The mean age was 61.8 years; 90 % were female, while 10 % were male. 80 % of the patients received the mRNA COVID-19 vaccine, while 20 % received other types. In addition, takotsubo cardiomyopathy (TCM) occurred in 50 % of patients receiving the first dose and another 40 % after the second dose of COVID-19 vaccines. Moreover, the mean number of days to the onset of symptoms was 2.62 days.
Global reports of takotsubo (stress) cardiomyopathy following COVID-19 vaccination: A systematic review and meta-analysis
https://www.sciencedirect.com/science/article/pii/S2352906722001579
Yet, what I find fascinating is that this VERY SAME syndrome is appearing in Long COVID!
Since the report of the first case from China in late 2019, the coronavirus disease (COVID-19) has spread very rapidly through the countries and regions leaving a trail of devastation in its path, everywhere. Although COVID-19 is primarily a respiratory illness mainly affecting the lungs; involvement of other organs including the cardiovascular system has been widely recognized. Whilst COVID-19 is an acute illness for a majority of cases; some of the debilitating virus-related symptoms can last for weeks and months, and are collectively termed as long COVID syndrome. Several published reports have described an association between acute COVID-19 illness and cardiac complications such as myocarditis and Takotsubo cardiomyopathy. However, little is known about any link between long COVID syndrome and the cardiac disease.
Long COVID Syndrome and Takotsubo Cardiomyopathy: An Unwelcome Combination
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8482351/
I believe I can shed light on the link between Long COVID and Takotsubo Cardiomyopathy. That link is NEUROINVASION. Takotsubo Cardiomyopathy can be caused by damage to the Amygdala.
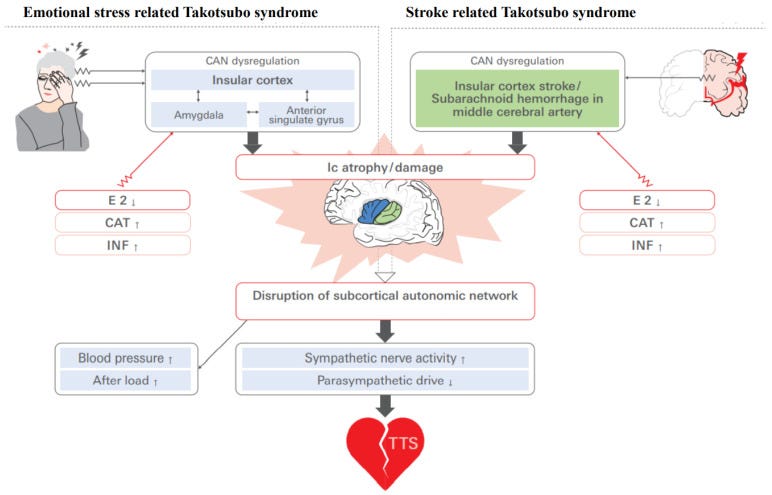
Takotsubo syndrome (TTS), a transient form of dysfunction in the heart’s left ventricle, occurs predominantly in postmenopausal women who have emotional stress. Earlier studies support the concept that the human circulatory system is modulated by a cortical network (consisting of the anterior cingulate gyrus, amygdala, and insular cortex (Ic)) that plays a pivotal role in the central autonomic nervous system in relation to emotional stressors.
Similar findings from the “acute spike protein death” (as I like to now call it), including the catecholamine surge are present.
And, as a very important note, is the following why women are more likely to have Long COVID?
Clinical studies revealed that damage involving the Ic is associated with QT prolongation, myocardial injury, and a higher plasma level of catecholamine; these conditions have also been observed in individuals with TTS [4].
Studies of gender-specific responses to changes in sympathovagal balance and asymmetry in cerebral function have suggested that a dominant pattern in females is determined by the left hemisphere, since functional cerebral asymmetry appears to be changed according to the body’s estrogen levels. The sympathovagal autonomic balance might be shifted via changes in CAN outflow due to functional cerebral asymmetry variability.
And here we have the definitive hallmarks of Acute Spike Protein Death and, perhaps, Long COVID!
Sympathetic autonomic nervous system overactivity is one possible pathophysiology underlying TTS. Elevated concentrations of plasma norepinephrine have been reported in acute stroke, and ECG changes in TTS were also observed after an intravenous or intracoronary injection of catecholamine. Increased sympathetic nervous system activity is an apparent link in the relationship between cerebrovascular disease and TTS specifically in postmenopausal women.
Sex Hormone-Specific Neuroanatomy of Takotsubo Syndrome: Is the Insular Cortex a Moderator?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8773903/
So, why am I convinced the Spike Protein is neurologically inducing this cardiac disease?
Because the AMYGDALA is precisely what SPED damages!
A paper from two weeks ago caused me to pursue this course of research. I have finally put it all together.
SUN CITY, Ariz. (Oct. 13, 2022) – A recent study conducted by Banner Sun Health Research Institute researchers has revealed new information and findings on how the COVID-19 virus invades the human brain. The study is the most comprehensive research on COVID-19 in the brain to date.
Researchers also found massive changes in the olfactory bulb and the closely-connected amygdala brain region. Aside from explaining the loss of the sense of smell in people with COVID-19, these changes could contribute to depression and other emotional changes in the weeks and months after infection.
New study reveals insights on effects of COVID-19 in the brain
https://www.bannerhealth.com/newsroom/press-releases/new-study-reveals-insights-on-effects-of-covid-19-in-the-brain
And, the Spike Protein, which disrupts the blood-brain barrier, and causes SPED, can directly cause this Amygdala-Hippocampus driven Sympathetic Overdrive.
The SARS-CoV-2 interactome has identified several antigens that may disrupt the blood-brain-barrier by inducing premature senescence in many cell types, including the cerebral endothelial cells. This enables the stress molecules, including angiotensin II, endothelin-1 and plasminogen activator inhibitor 1, to aberrantly activate the amygdala, hippocampus, and medial prefrontal cortex, increasing the vulnerability to stress related disorders.
PTSD as an Endothelial Disease: Insights From COVID-19
https://www.frontiersin.org/articles/10.3389/fncel.2021.770387/full
Which brings me to my next topic of research. Is Long COVID a combination of microvascular destruction and constant sympathetic overdrive?
thanks walter for all your dedication and hard work, and please, please do not give up on us.
even if we do not know realize it yet, we need you!!
This is a serious question. We repeatedly hear about the mysterious (at least to me) problem of 'Long Covid'. Leaving apart the fact I believe it's often a case of 'Long Vaccine', can someone explain how it works ... if you go to a doctor with a case of, for example, myocarditis, as a result of Covid (or a side effect of the vaccines but thats another matter), what are you suffering from, Long Covid or myocarditis? I feel L/Covid is being used as a catch all when it might make more sense to say you have "Covid induced myocarditis", or "vaccine induced myocarditis", not the vague "Long Covid" which could be just about anything - or nothing