

New Onset Autoantibodies After Any Exposure to the Spike Protein of SARS-CoV-2
Evidence proving my hypothesis from 2020 that molecular mimicry of the Spike Protein is inducing autoimmune disease.

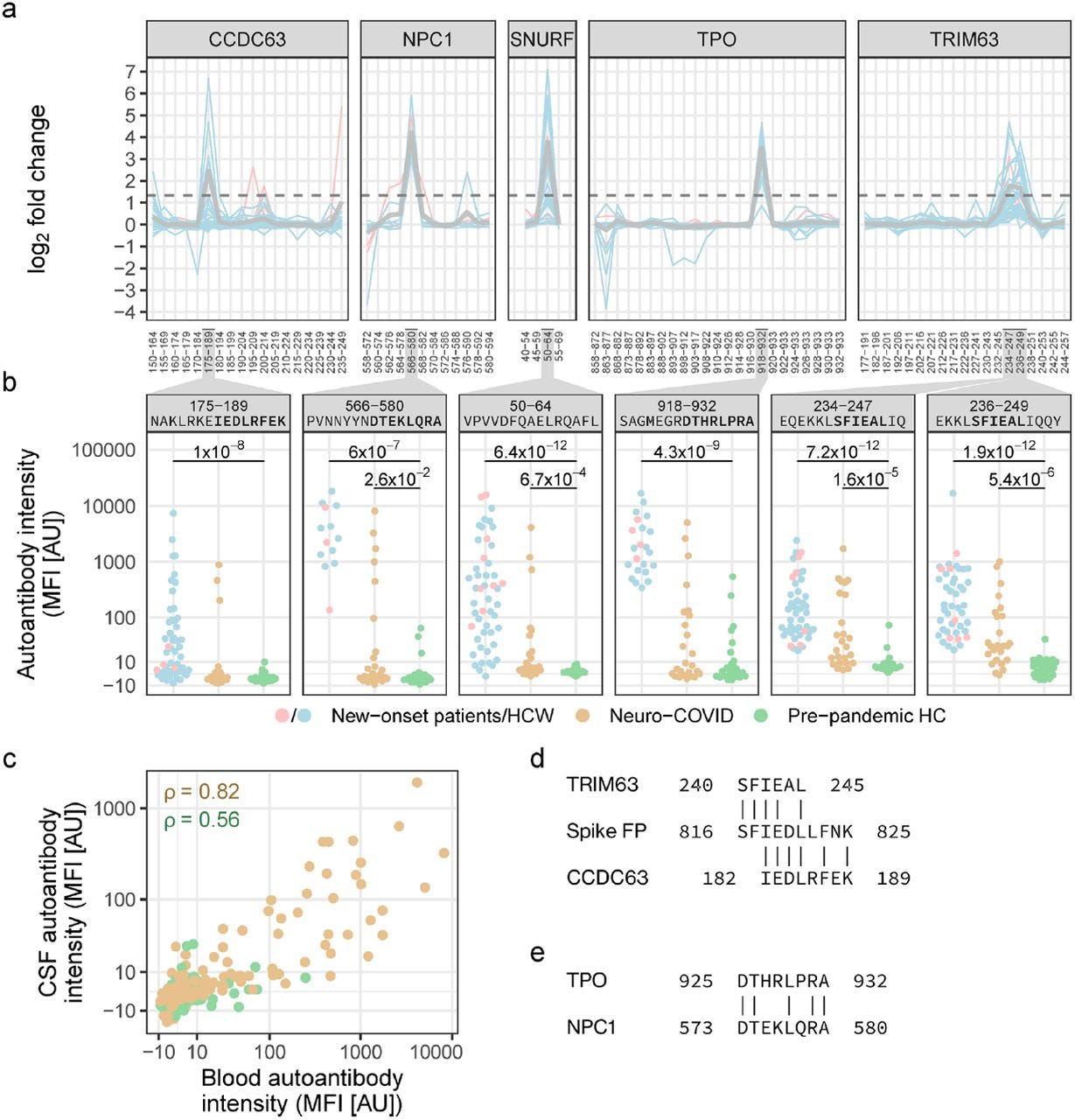
The main epitopes of new-onset autoantibodies are elevated in blood and CSF of an independent cohort with neuro-COVID and display molecular mimicry with the SARS-CoV-2 fusion peptide.
a Epitope mapping revealed the main epitopes of six new-onset autoantibodies. Lines depict epitope profiles (anti-peptide IgG log2 FC) at new-onset in individuals with the corresponding new-onset autoantibody. Gray lines depict the mean. The dashed line indicates the cutoff for classification as a main epitope (FC≥2.52). Numbering on the x-axis corresponds to the peptide amino acid positions in the full-length protein (Table S3). b Antibodies against the main epitopes were elevated in an independent cohort of neuro-COVID patients compared to pre-pandemic HCs. Brackets indicate statistically significant difference to pre-pandemic HC (q-values ≤ 0.05 from Mann-Whitney U-test with Benjamini-Hochberg correction). The y-axis displays signal intensity on the pseudo-log10 scale. c Correlation of autoantibodies in blood and CSF of neuro-COVID patients and pre-pandemic HCs. Data points correspond to paired blood and CSF samples in neuro-COVID patients (n=23) and HCs (n=21), and the peptides shown in panel b. ρ: Spearman’s rho. d,e Sequence similarity between d the main epitopes of TRIM63 and CCDC63 to the SARS-CoV-2 fusion peptide, and e between the main epitopes of TPO and NPC1.
Those who have followed my research into COVID19 from the beginning will know that in 2020 I hypothesized and warned that the molecular mimicry between the Spike Protein and human antigens would inevitiably induce autoimmune disease.

This has, unfortunately, been proven to be correct. As mentioned above, I literally begged the authorities to halt the Spike Protein injections as I was certain autoimmune disease would occur. The mechanism, at least to me, is as clear two plus two equals four. The evidence for this outcome was that obvious.
A preprint, which was published February 15th of this year, has shown that this molecular mimicry induced autoimmune disease is occurring. What is most interesting about the study is that new onset autoantibodies appear to be occurring in three distinct patterns: stable, transient and delayed onset. The delayed onset category is particularly concerning as these autoantibodies occurred in many post-vaccination.
The dynamics of detected new-onset autoantibodies followed three distinct patterns: stable, transient, and delayed onset. The acute onset types reflect autoantibody persistence, while delayed onset may reflect other parameters. As 31% (49 of 159) of delayed new-onset autoantibodies emerged in individuals who were vaccinated between seroconversion and the subsequent visit, the onset of these autoantibodies may be vaccine associated.
Among the new onset autoantibodies discovered, three are involved in skeletal muscle, heart and brain functioning. These are, of course, three fundmamental sources of Long COVID pathology. Most likely part of the "sudden death" puzzle we are all striving to solve.
Since neurological symptoms after COVID-19 are commonly occurring and often debilitating, we made directed efforts in understanding this group of symptoms post-COVID-19. We found three new-onset autoantibodies connected to increased severity of neuropsychiatric symptoms post-COVID-19: anti-CALU, MYO16, and SNURF IgG. CALU is a membrane-bound or secreted calcium-binding protein mainly expressed in heart and skeletal muscle. MYO16 is a cytoplasmic unconventional myosin with enhanced brain expression, and may be involved in the extension of neuronal membrane processes36. SNURF is a small (71 aa) nuclear protein of unknown function, primarily expressed in brain and muscle tissues and cardiomyocytes. In addition, we found associations of 11 self-assessed non-neurological symptoms post-COVID-19 to 8 of the most prevalent new-onset autoantibodies. However, these associations were tentative, with only the association of anti-PCYT1B IgG and impaired hearing remaining significant after FDR correction.
Despite not showing any clear molecular mimicry with SARS-CoV-2, anti-SNURF IgG emerged in 9% of HCW (n=40) and 20% of hospitalized COVID-19 patients (n=9). Furthermore, anti-SNURF|50-64 IgG was significantly elevated in patients with neuro-COVID compared to pre-pandemic HCs. It is worth noting that SNURF, like the other two most prevalent autoantibody targets TRIM63 and CCDC63, is expressed in heart (SNURF and TRIM63) and skeletal muscle. In addition, SNURF is expressed in several other tissues including the brain, corroborating the association of anti-SNURF IgG and neuropsychiatric symptoms post-COVID-19. Like CCDC63 and many classical autoantigens, SNURF is located to the nucleus indicating that epitope spreading may be the source of anti-SNURF IgG39. Furthermore, anti-SNURF IgG was the most common autoantibody increasing at vaccination.
But, where do they originate from? How do they occur? The answer is precisely what I predicted: it is from molecular mimicry of the Spike Protein.
Our epitope mapping identified the main epitopes of five new-onset autoantibodies. The epitopes for TRIM63 and CCDC63 displayed an alignment to the fusion peptide of the SARS-CoV-2 spike glycoprotein. The fusion peptide is crucial for viral entry and is highly conserved across coronaviruses. Interestingly, two other studies independently found that human antibodies that broadly neutralize coronaviruses are targeting the fusion peptide. In addition, Spike ACE2 binding was shown to expose the fusion peptide to these antibodies37. However, we showed that there is no correlation between anti-SARS-CoV-2 IgG and general new-onset autoantibody signals, suggesting that there may be additional mechanisms behind new-onset autoantibodies aside from cross-reactivity of anti-SARS-CoV-2 IgG, such as epitope spreading by, e.g., bystander tissue destruction or intramolecular linkage.
Prevalent and persistent new-onset autoantibodies in mild to severe COVID-19
https://www.medrxiv.org/content/10.1101/2024.02.15.24302857v1.full-text
As noted above, another point I was correct about, reinfections are indeed common and can occur in rapid succession. Will repeated exposure to the Spike Protein eventually induce these autoantibodies in an ever increasing percentage of the population? We need continual monotoring of these patients, and of the general population, to determine if this may be the case.
I will continue my work on ways to prevent and ameliorate the damage done by this, in my opinion, clearly created pathogen. Thank you for your readership, support and dialog. It is what makes my work possible. Helping all of us is what makes it worthwhile.
Walter, whenever your newest post shows up in my mailbox, no matter what I am doing I immediately stop literally everything & anything to strap myself in the chair, open, and dive in. This one was certainly no exception, and at the very least confirms the phenomenon & identifies key mechanisms by which autoimmune disease is manifesting as a result of both infection and injection. Cannot overstate how impactful your work has been to me, nor how illuminating your insights. The final point you made (in the next to last paragraph) perfectly articulates one of my own greatest ongoing concerns/questions: "Will repeated exposure to the Spike Protein eventually induce these autoantibodies in an ever increasing percentage of the population? We need continual monitoring of these patients, and of the general population, to determine if this may be the case." I fear the answer is what we already, at the very least, strongly suspect if not "know". Time will unavoidably reveal the inevitable beyond any doubt. Thank you yet again for your incredible and utterly unsurpassed work.
Walter, may I suggest you look at D3 as a way to both prevent infection, and to prevent re-infection. I know a few people with high D3 levels (as in 85 to 100 ng/ml), who just don't get sick. I'm one of them. It does really work, and costs pennies per day.