

Mellor-Pita et al., (July 3rd) Provide Convincing Evidence for My 2020 Hypothesis that the Spike Protein Induces Catastrophic Antiphospholipid Syndrome (CAPS)
Is CAPS an eventual common complication (fate?) from repeated infections/exposures to the Spike Protein?

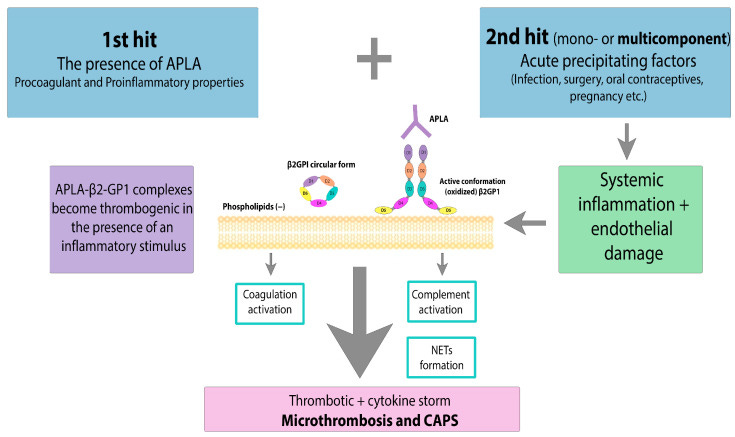
CAPS: the “two-hit” theory. APLA—antiphospholipid antibody, β2GPI—β2-glycoprotein I. Acute precipitating factors as a 2nd hit lead to systemic inflammation and endothelial damage. Massive cytokine release, NET formation and coagulation activation result in microthrombosis and CAPS.
BEFORE the vaccines were released I sent out an alarm to many very high-level immunologists. I will not reveal their names, but I will share one of those emails with the recipient’s name redacted. Of course, I was met with: The vaccines are safe and none of this can happen. Not ONE. Not one high-level immunologist shared my concerns. Indeed, my concerns were dismissed.
Here is that email:
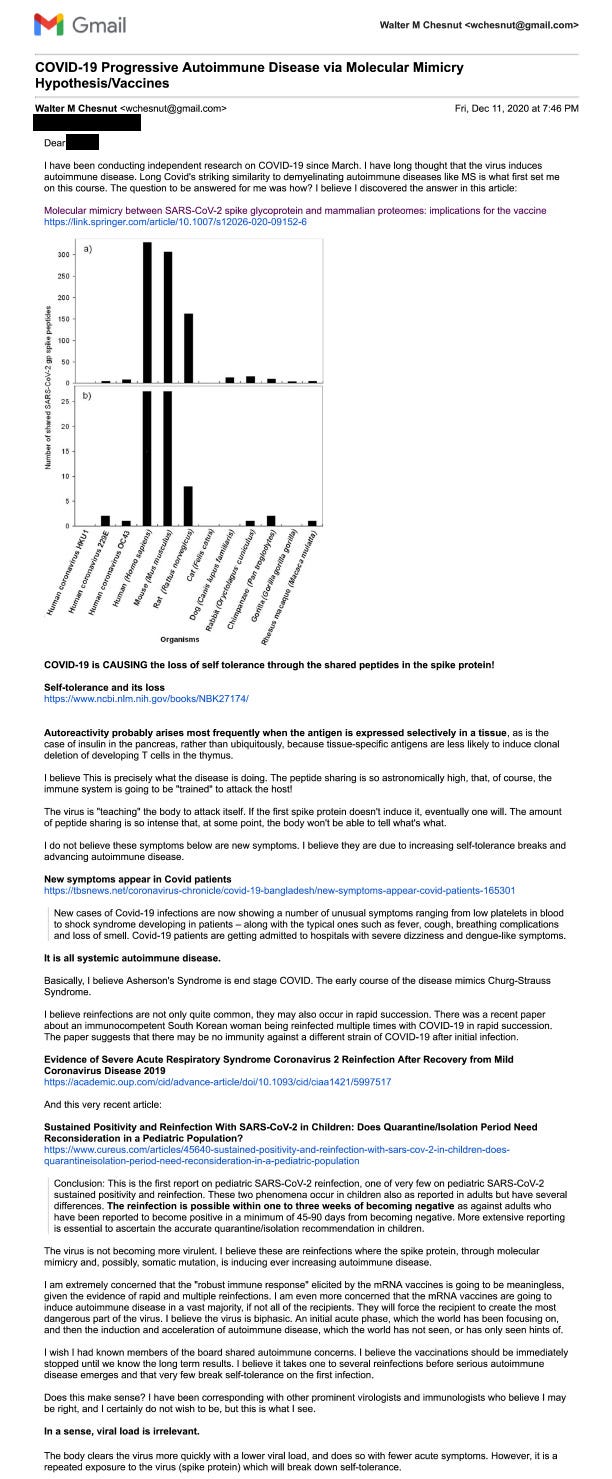
The critical point of the email is the following statement:
Basically, I believe Asherson’s Syndrome (CAPS) is end-stage COVID. The early course of the disease mimics Churg-Strauss Syndrome.
END STAGE COVID AND ASHERSON’S SYNDROME
https://wmcresearch.org/end-stage-covid-and-ashersons-syndrome/
Now, my hypothesis is based on molecular mimicry, which is a CAPS development mechanism.
Molecular mimicry is one of the CAPS development mechanisms. According to research results, a number of microorganisms contain special sequences in their genetic material that are similar to the sequences in the binding site of β2GPI with phospholipids, resulting in cross-reactivity with the own structures.
Catastrophic Antiphospholipid Syndrome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10779422/
And here is where the recent paper becomes very important. Anti-β2GPI is PRECISELY the antibody being found in severe COVID cases.
A total of 29 patients (18.2%) and 14 healthy donors (17.5%) were positive for aPL. Nineteen COVID-19 patients (12%) but no healthy donor presented a positive percentage of the IgA isotype aPL. IgA anti-β2-glycoprotein I antibodies (anti-β2GPI) were the most frequent type (6.3%) in patients but was not detected in any healthy donor. The positivity of this antibody was found to be significantly elevated in patients with thromboembolic events (25% vs. 5%, p = 0.029); in fact, patients with positive IgA anti-β2GPI had an incidence of thrombosis over six times higher than those who had normal antibody concentrations [OR (CI 95%) of 6.67 (1.5–30.2), p = 0.014]. Additionally, patients with moderate-severe disease presented a higher aPL positivity than patients with mild disease according to the Brescia (p = 0.029) and CURB-65 (p = 0.011) severity scales. A multivariate analysis showed that positivity for IgA anti-β2GPI is significantly associated with disease severity measured by CURB-65 [OR (CI 95%) 17.8 (1.7–187), p = 0.0016].
IgA Anti-β2-Glycoprotein I Antibodies as Markers of Thrombosis and Severity in COVID-19 Patients
https://www.mdpi.com/1999-4915/16/7/1071
Now, let’s go back to CAPS. One of the prerequisites for CAPS to develop is the presence of these antibodies. Please see the above graphic.
Yes. The connection between COVID (the Acute Precipitating Factor) and CAPS has been made. (Isn’t it fascinating! SARS-CoV-2 (almost certainly) induces the prerequisite autoantibodies and provides the trigger for CAPS!)
A severe SARS-CoV-2 infection is characterized by an hyperinflammatory reaction, endothelial dysfunction and systemic microthrombosis followed by multiple organ failure, increased ferritin, and other indicators, which are associated with high mortality among patients [100]. Clinical manifestation of thrombophilia that occurs during severe SARS-CoV-2 infection is similar to the symptoms of CAPS. SARS-CoV-2 can lead to the development of CAPS in APS-positive patients due to indirect activation of complement and the associated procoagulant state [101]. The mechanisms of hemostasis disorders in severe SARS-CoV-2 infection and CAPS are diverse and similar at the same time. There is often simultaneous activation of many pathways, including activation of platelets, external and internal pathways of coagulation cascade, suppression of fibrinolysis, etc. with the development of DIC, thrombotic microangiopathy, and even local intravascular coagulation in the lungs. Poorly controlled inflammation and hyperactivation of blood clotting cause not only a cytokine storm but also a thrombotic storm in severe COVID-19 and CAPS.
Followed by this rather ridiculous (in my opinion) statement:
At the same time, ferritin, being a marker of SARS-CoV-2 severity, is also elevated in many patients with CAPS. SARS-CoV-2 can lead to disruption of the cytokine response, but the development of autoimmunity in patients with coronavirus infection is still a matter of debate.
Catastrophic Antiphospholipid Syndrome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10779422/
To bring the conversation full circle: What I observed in 2020 was that the molecular mimicry of the Spike Protein would cause systemic autoimmune disease. The most immediately devastating of which would be CAPS. As the evidence pours in, there is a significant amount that points to this. I believe we need screening in the general population as well as those who are suffering from repeated infections to determine the presence and level of these antibodies and their trends over time.
Thank you, as always, for your support, dialog and readership. If you are in the Northeast of the States, please try to keep cool.
So I was sent to ATAGi Infectious diseases Dr as a healthcare worker refusing this as a significant past history of clots, last one a saddle PE which put me ICU post a torn calf muscle.
This Dr blatantly told me he can not provide me with an exemption and only condition that is considered contraindicated was antiphosphid lipid syndrome which triggered my memory which I said oh I was diagnosed with this in my last pregnancy, which he then dismissed I’m sure thinking I made this up. No tests offered, no let’s get your history and check told good sorry you won’t be able to work in health, good luck. This pretty much confirmed this is a genocide with massive gaslighting I had never seen in 25 years as a health worker. But it also tells me they knew this.
Antiphospholipid Syndrome caused by Endotoxin in Covid19 Jabs
https://geoffpain.substack.com/p/antiphospholipid-syndrome-caused