


LIES. IT WAS NEVER “PNEUMONIA.” COVID-19 ARDS IS DUE TO DAMAGED PULMONARY CAPILLARY ENDOTHELIUM: THE IMPORTANCE OF GROUND GLASS OPACITIES (GGO)
COVID-19 ARDS mimics Paraquat Poisoning due to the Spike Protein’s interaction with the capillary endothelium

It is important to understand that the entire early response to COVID-19 was DISASTROUSLY wrong. I knew it wasn’t a traditional “pneumonia,” but did not know enough (none of us uninvolved with the WHO did then) to determine exactly what was occurring in the lungs. However, I am ALMOST CERTAIN that there are those that DID KNOW and allowed for FATAL “treatment” regimens to be implemented.
THE ARDS EVIDENT IN COVID-19 IS DUE TO THE SPIKE PROTEIN (SPED) DAMAGING THE PULMONARY CAPILLARY ENDOTHELIUM, PRECISELY IN THE SAME WAY PARAQUAT (PQ) POISONS THE LUNGS
How does this occur? PQ generates HUGE AMOUNTS OF ROS! EXACTLY THE SAME AS THE SPIKE PROTEIN!
Paraquat (PQ; 1,1-dimethyl-4,4-bipyridinium dichloride) is a highly toxic herbicide to humans. Acute PQ poisoning during suicide attempts or after accidental ingestion causes a high mortality (50–90%) because of a lack of effective treatment or an antidote. A uniformly used prognostic indicator that reliably predicts the risk of death at an early stage in poisoning is of great importance in assessing clinical benefit from various interventions. The main target organ for PQ toxicity is the lung as a consequence of PQ accumulation against a concentration gradient through the highly developed polyamine uptake system, and due to its capacity to generate huge amounts of pro-oxidant reactive species through a strenuous redox-cycle pathway.
The Volume Ratio of Ground Glass Opacity in Early Lung CT Predicts Mortality in Acute Paraquat Poisoning
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0121691
Now, let us look at the pathology that occurs in COVID-19 ARDS.
For example, viral damage to alveolar type II cells will lead to flooding of airspaces because the water-tight air-blood barrier is broken. This damage may be exacerbated because alveolar type II cells also produce lung surfactant. Reduced lung surfactant will lead to collapsed alveoli and reduced surface area for gas exchange. However, a hyperactive immune response will lead to an excessive accumulation of inflammatory cells, such as macrophages and neutrophils, which further increases the fluid permeability of the air-blood barrier and cell damage (Mirad & Martin; 2020).
Coronavirus ARDS (CARDS) - Healing a Broken Lung
https://www.criver.com/eureka/coronavirus-ards-cards-healing-a-broken-lung
Returning to Paraquat Poisoning, Please note that IT IS EXACTLY(!!!) THE SAME PATHOLOGY!!!!!!!!!!!
It is well-known that the main target organ for PQ toxicity is the lung. The pulmonary lesion has two phases, acute alveolitis followed by secondary fibrosis. In the alveolitis phase, the air-blood barrier is destroyed; type I and II pneumocytes swelling, thus the gas exchange between the air space and the capillaries is destroyed and the surface tension within the alveoli is increased, causing edema of capillaries. Damaged pulmonary capillary endothelium leads to pulmonary hemorrhage or edema and infiltration in the interstitial tissue and air spaces of the lung with inflammatory cells. The onset of the proliferative phase occurs several days after PQ ingestion. The normal architecture of the lung is destroyed due to the proliferation of fibroblasts and deposition of collagen, thereby reducing the effectiveness of gaseous exchange, leading to death as a consequence of severe anoxia. In a previous study, the GGO lesion appears during the damage stage and reflects alveolar edema and inflammatory cell infiltration, thus indicating primary alveolitis from PQ. Therefore, the quantitative GGO lesion may represent the extent of alveolitis and could predict the risk of death in the early stage.
The Volume Ratio of Ground Glass Opacity in Early Lung CT Predicts Mortality in Acute Paraquat Poisoning
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0121691
So, please note again, in the pathology of PQ poisoning:
…the GGO lesion appears during the damage stage and reflects alveolar edema and inflammatory cell infiltration, thus indicating primary alveolitis from PQ.
This indicates that the Ground Glass Opacities observed in COVID-19 ARE NOT FROM “PNEUMONIA!” They are from DAMAGED ALVEOLI DUE TO THE SPIKE PROTEIN DAMAGING THE PULMONARY CAPILLARY ENDOTHELIUM!
This can be proven.
Based on our data and the available published studies, we can infer that, during the early phase of the infection, the lung microvasculature is the first target of SARS-CoV-2. Indeed, the high replication rate of the virus in lung epithelial cells could particularly affect the local microvascular endothelial cells lining the capillaries in the alveoli. Overall, we demonstrate that SARS-CoV-2-derived S1 is sufficient in itself to propagate inflammatory and thrombogenic processes in the microvasculature, amplified by the complement system, recapitulating the thromboembolic complications of COVID-19..
SARS-CoV-2 Spike Protein 1 Activates Microvascular Endothelial Cells and Complement System Leading to Platelet Aggregation
https://www.frontiersin.org/articles/10.3389/fimmu.2022.827146/full
What is important to remember in all of this is that ARDS is the result of INJURY! Not necessarily VIRUS!
Pathologically, ARDS is characterized by diffuse alveolar damage, which is created by abnormal alveolar-capillary permeability, resulting in an influx of protein and fluid into the alveoli and interstitial spaces. This process is caused by alveolar injury secondary to one (or more) of many precipitating insults, including sepsis and toxic inhalational injuries. Ensuing fibrin deposition and collagen formation can lead to pulmonary fibrosis.
There is usually a radiographic latent period in the first 24 hours following the initial insult that causes ARDS, and the chest radiograph is frequently normal.4 The exception is if ARDS is triggered by a direct lung injury (for example pneumonia), in which case consolidation may be observed. There is rapid deterioration in the subsequent 24–72 hours. Injury to the endothelium results in increased capillary permeability and the influx of protein-rich fluid into the alveolar space and interstitium, which promotes pulmonary edema. Air space and interstitial opacities on the chest radiograph in ARDS are predominantly bilateral and symmetrical.
Imaging of Acute Respiratory Distress Syndrome
https://rc.rcjournal.com/content/57/4/607
So, what convinces me that COVID-19 “Pneumonia” is not “Pneumonia” at all? THE PRESENCE OF PNEUMOMEDIASTINUM! This is present in INJURY, such as PQ poisoning, but is RARE in VIRAL PNEUMONIA!
Spontaneous pneumomediastinum is uncommon in viral pneumonia.
Spontaneous pneumomediastinum in COVID-19
https://casereports.bmj.com/content/13/5/e236519
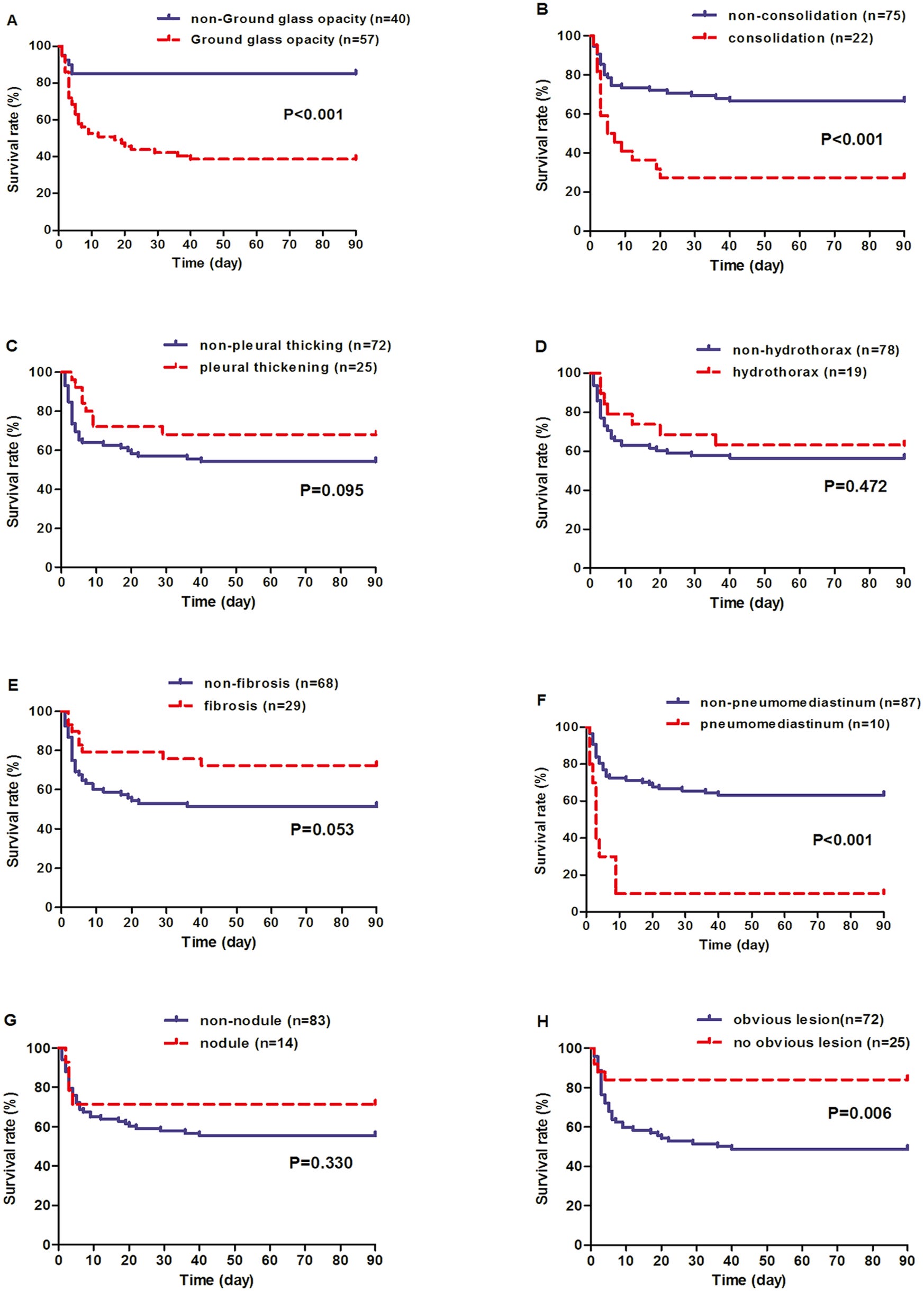
Of 97 patients, 41 (42.3%) died. Among the eight different types of lung CT findings which appeared in the first 5-day of PQ intoxication, four ones discriminated between survivors and non-survivors including ground glass opacity (GGO), consolidation, pneumomediastinum and “no obvious lesion”.
The Volume Ratio of Ground Glass Opacity in Early Lung CT Predicts Mortality in Acute Paraquat Poisoning
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0121691
However, it is common in COVID-19 “Pneumonia!’
There is an emerging understanding that coronavirus disease 2019 (COVID-19) is associated with increased incidence of pneumomediastinum.
Pneumomediastinum in COVID-19: a phenotype of severe COVID-19 pneumonitis? The results of the United Kingdom (POETIC) survey
https://erj.ersjournals.com/content/early/2022/01/27/13993003.02522-2021
Ah, yes, we have been lied to. Lies, lies, lies.











Wow. In early January 2022 I came down with a whopping case of the COV. High fever, cough, tachycardia. Went to the ER: CT scan showed bilateral symmetrical ground glass opacity "pneumonia"; serum elevated D-Dimer & troponin & LDH & ferritin, and of course a + COV test. Luckily my O2sat stayed at 93 so I was admitted but not vented. Also had vertigo and severe weakness, no taste & smell, and no saliva. NOT jabbed. Sent home after 5 days, slightly improved. Needed a walker for another week. Very gradual recovery and I was close to normal by spring. I think I am lucky to have survived and not been "treated", especially as I am over 65yo.
This article is particularly relevant to me. I can tell you for sure it was not a bad cold or flu! I'm most grateful for your work, and I am confident I know more than the average PCP from reading your & your colleague's substacks.
The truth becomes more revealing as to the diabolical intent of the “public health” alphabet criminals. The lies were to cover their plan of torture and mass murder. Thank you for explaining the truth so we can hold the sociopaths accountable.