

Lessons from Bloodwork: How the Spike Protein Mimics HIV Infection
Unknown to many, SARS-CoV-2, like HIV, targets gut CD-4 cells.

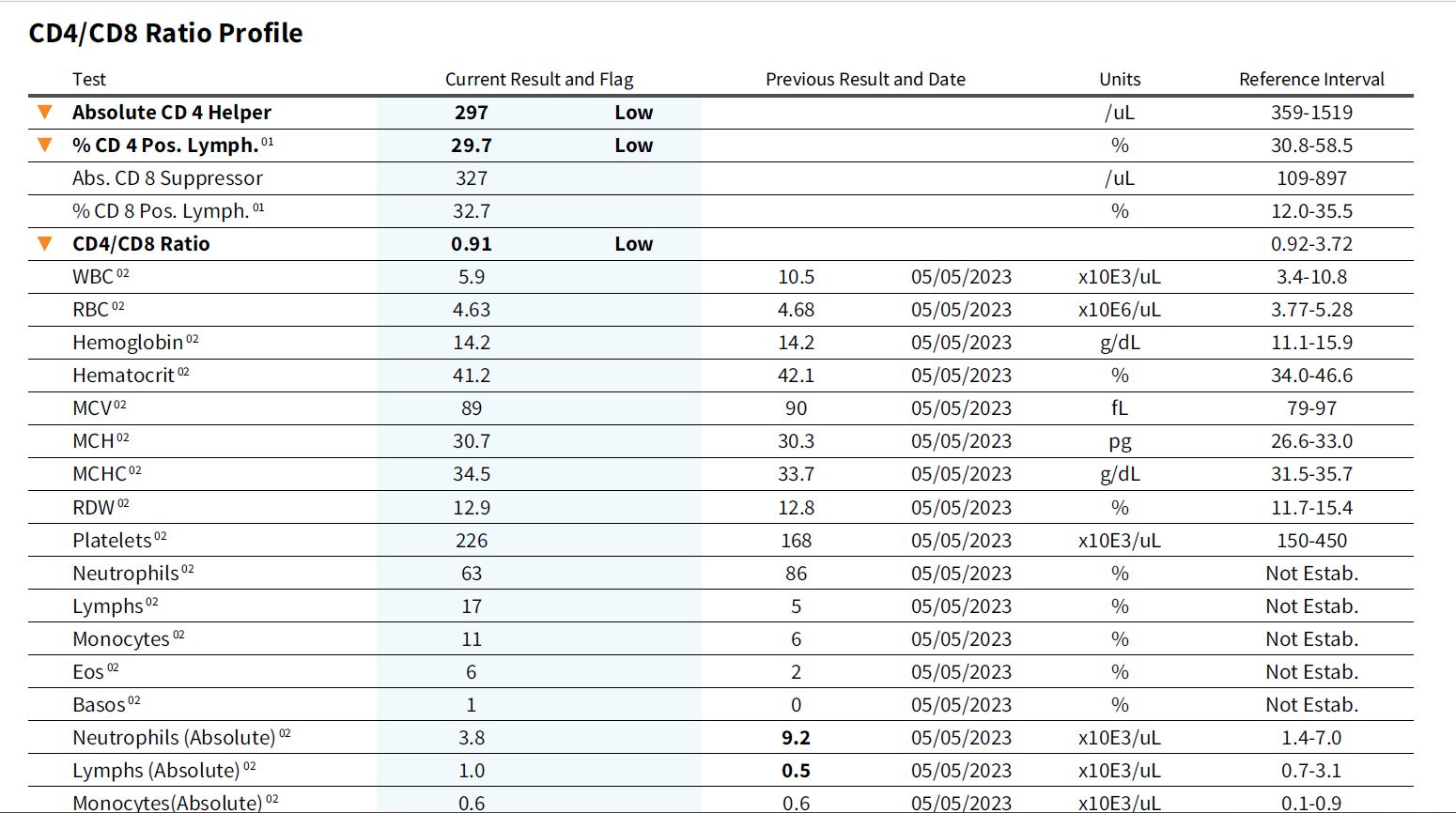
I read a post on X over the weekend which disturbed me greatly and caused me to delve deeply into the mechanisms of HIV. An HIV neg patient presented with a low CD4 cell count. This patient had COVID and was fully vaccinated. The doctor who posted the bloodwork commented that this finding “is more common than people want to believe.” The image above are the results of that bloodwork.
I couldn’t agree more with the doctor. In fact, as I have been warning for years, the mild symptoms that most experience from a COVID infection may not tell the full story of a COVID infection. After all, HIV is very similar in that the initial acute phase of the disease is very mild or virtually asymptomatic.
Let’s start with something HIV does which is very relevant in the context of SARS-CoV-2. This is the unknown-to-most fact that HIV shows a more serious depletion of CD4 T cells in the guy than in the blood. Also, like SARS-CoV-2, HIV triggers chronic immune activation.
HIV infection is associated with a progressive decline of circulating CD4+ T cells and loss of immune functions; however this infection shows a more severe depletion of CD4+ T cells in the gastro-intestinal tract than in blood [22,23,162]. In the acute phase of infection, the virus depletes CD4+ T cells in the mucosal tissue of the gut as they represent the “ideal targets” of the virus (activated CD4+ T cells, near the front door of the virus, at the lining of the vagina or anus). In this process, the virus also destroys the gut mucosas‘s structural cells, allowing gut bacteria or other pathogens to penetrate the body; these phenomena lead to irreversible damage to the immune system. Finally, HIV triggers chronic immune activation. Recently, a strong association between the destruction of intestinal CD4+ T cell homeostasis in the gut and the level of systemic CD4+ T cell activation [162] has been described.
CD4+ T Cell Depletion in Human Immunodeficiency Virus (HIV) Infection: Role of Apoptosis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3185763/
In SARS-CoV-2 infection, we have, in essence, the precise same situation occurring in the gut. This is in regards to inflammation and CD4 counts.
Multiple components of the gut immune system are affected, resulting in a diminished or dysfunctional gut immunological barrier. Antiviral peptides, inflammatory mediators, immune cell chemotaxis, and secretory immunoglobulins are important parameters that are negatively affected in SARS-CoV-2 infection. Mucosal CD4+ and CD8+ T cells, Th17 cells, neutrophils, dendritic cells, and macrophages are activated, and the number of regulatory T cells decreases, promoting an overactivated immune response with increased expression of type I and III interferons and other proinflammatory cytokines. The changes in the immunologic barrier could be promoted in part by a dysbiotic gut microbiota, through commensal-derived signals and metabolites. On the other hand, the proinflammatory intestinal environment could further compromise the integrity of the intestinal epithelium by promoting enterocyte apoptosis and disruption of tight junctions.
Exhaustion/depletion of CD4+ T cells, a hallmark of HIV infection, is also observed in SARS-CoV-2 infection. The resulting dysregulation of CD4+ T cells in the gut may contribute to intestinal epithelial barrier dysfunction and leaky gut, which promotes systemic inflammation (35). Accordingly, IL-17 producing Th17 cells are overactivated in SARS-CoV-2 infection (36).
Alterations in gut immunological barrier in SARS-CoV-2 infection and their prognostic potential
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10050566/
There is much evidence that the Spike Protein alone may be inducing these responses.
Studies have reported the occurrence of gastrointestinal (GI) symptoms, primarily diarrhea, in COVID-19. However, the pathobiology regarding COVID-19 in the GI tract remains limited. This work aimed to evaluate SARS-CoV-2 Spike protein interaction with gut lumen in different experimental approaches. Here, we present a novel experimental model with the inoculation of viral protein in the murine jejunal lumen, in vitro approach with human enterocytes, and molecular docking analysis. Spike protein led to increased intestinal fluid accompanied by Cl− secretion, followed by intestinal edema, leukocyte infiltration, reduced glutathione levels, and increased cytokine levels [interleukin (IL)-6, tumor necrosis factor-α, IL-1β, IL-10], indicating inflammation. Additionally, the viral epitope caused disruption in the mucosal histoarchitecture with impairment in Paneth and goblet cells, including decreased lysozyme and mucin, respectively. Upregulation of toll-like receptor 2 and toll-like receptor 4 gene expression suggested potential activation of local innate immunity. Moreover, this experimental model exhibited reduced contractile responses in jejunal smooth muscle. In barrier function, there was a decrease in transepithelial electrical resistance and alterations in the expression of tight junction proteins in the murine jejunal epithelium. Additionally, paracellular intestinal permeability increased in human enterocytes. Finally, in silico data revealed that the Spike protein interacts with cystic fibrosis transmembrane conductance regulator (CFTR) and calcium-activated chloride conductance (CaCC), inferring its role in the secretory effect. Taken together, all the events observed point to gut impairment, affecting the mucosal barrier to the innermost layers, establishing a successful experimental model for studying COVID-19 in the GI context.
SARS-CoV-2 Spike protein triggers gut impairment since mucosal barrier to innermost layers: From basic science to clinical relevance
https://www.sciencedirect.com/science/article/pii/S1933021924000291
And, perhaps more disturbingly, the gut may be a reservoir (along with many other locations) for persistent Spike production after natural infection.
SARS-CoV-2 viral rebound in the gut, possibly resulting from viral persistence, has also been associated with lower levels and slower production of receptor-binding domain IgA and IgG antibodies51. There are major differences in antibody creation, seroreversion and antibody titre levels across the sexes, with women being less likely to seroconvert, being more likely to serorevert and having lower antibody levels overall52,53, even affecting antibody waning after vaccination54.
Several reports have pointed towards possible viral persistence as a driver of long COVID symptoms; viral proteins and/or RNA has been found in the reproductive system, cardiovascular system, brain, muscles, eyes, lymph nodes, appendix, breast tissue, hepatic tissue, lung tissue, plasma, stool and urine55–60. In one study, circulating SARS-CoV-2 spike antigen was found in 60% of a cohort of 37 patients with long COVID up to 12 months after diagnosis compared with 0% of 26 SARS-CoV-2-infected individuals, likely implying a reservoir of active virus or components of the virus16. Indeed, multiple reports following gastrointestinal biopsies have indicated the presence of virus, suggestive of a persistent reservoir in some patients58,61.
Long COVID: major findings, mechanisms and recommendations
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9839201/
Please remember, before we figured out what was really going on with HIV, we opened Kaposi Sarcoma clinics, noticed rare cancers and pneumonias. All eerily similar to what is happening now.
Nonetheless, we will continue to search for treatments and preventative measures. It is, however, beyond unfortunate that we have been put into this situation by almost certainly artificial means.
Thank you, as always, for your continued support, readership and dialog.
VAIDS. I’ve been screaming this for 3 years, and this is what led to my father’s death. I requested a lymphocyte test in 2021, for my dad, and told the doctors at the VA I felt strongly the Covid gene therapy death shots had caused my dad’s health to rapidly deteriorate. No one listened, they looked at me like I was crazy. I ended up sharing his results on Infowars, live on air… We must continue to be a light and shine the truth for all to see.
Wasn’t it found that HIV was inserted into the virus? Perhaps thst is the reason Covid is mimicking the symptoms of AIDS?