

J’ACCUSE! THE SPIKE ANTIBODY/FC-RECEPTOR COMPLEX IS SOURCE OF SEVERE COVID AND THE INDUCTION OF SYSTEMIC AUTOIMMUNE DISEASE: ONE SIDE OF THE AUTOIMMUNE/AMYLOIDOSIS SARS-CoV-2 COIN - AND IT WAS KNOWN!
Paper Published Feb 2020 by Shi Zhengli (clearly written before pandemic appeared) as Smoking Gun

I believe I have discovered the mechanism by which the Spike Protein is causing severe disease and autoimmune disease. In both cases, the mechanism is the same. Autoimmunity and Amyloidosis are the two sides of the SARS-CoV-2 coin. And they are present in both the acute phase and the so-called Long COVID (or PASC) phase (rapid and indolent, respectively).
THE HISTORY
In June 2018, a paper was published in the Hong Kong Medical Journal called Antibody-dependent enhancement of SARS coronavirus infection and its role in the pathogenesis of SARS. The paper has a very interesting Discussion:
The findings of this study partially invalidated our initial hypothesis that antibody-mediation would, by widening tropism of SARS-CoV toward immune cells, elicit an altered profile of immune mediators that impair homeostasis of the immune system and ultimately contribute to SARS pathogenesis.
BUT! In the very next sentence, the authors go on to say:
Nonetheless, it is still intriguing to us that triggering an enhanced infection of cornerstone innate immune cells such as macrophages would have no consequences. It is true that in contrast to studies that showed cell perturbation following ADE-infection, others have documented fewer, barely discernible consequences. Hence it is possible that ADE of SARS-CoV infection is happening without deleterious consequences to the target cells.
The paper then concludes:
Our results suggest the rational development of vaccination strategies in the event of a SARS-like virus outbreak, with reasonable concerns about the occurrence of severe adverse effects.
MOVE AHEAD TO FEBRUARY 2020, MERE WEEKS BEFORE THE PANDEMIC WAS DECLARED
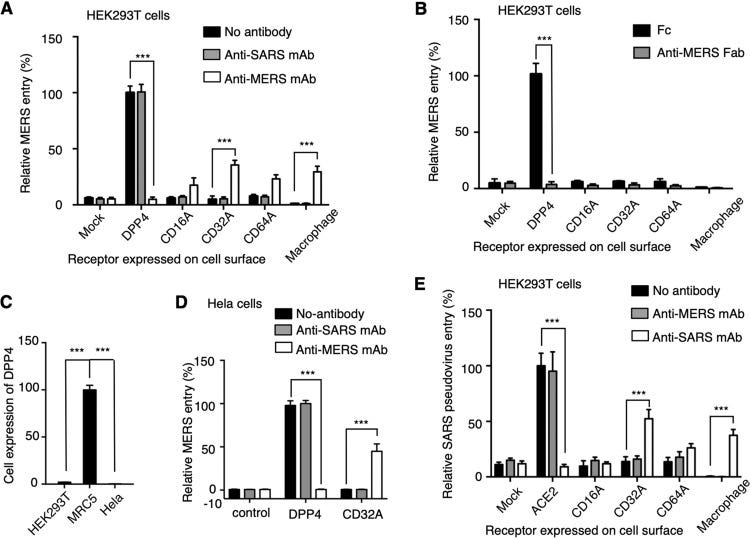
A PAPER PUBLISHED BY NONE OTHER THAN SHI ZHENGLI MADE THE FOLLOWING DISCOVERY:

The authors found that MERS-CoV and SARS-CoV DO have Fc receptor mediated and DOSAGE DEPENDENT mediated Antibody Dependent Enhancement (ADE)! This may, at long last, explain why there seems to be more severe disease at points post vaccination and why, if the virus is not cleared, the DOSAGE of antibodies within the body from infection can then cause progression of the disease! (Please note the mention of the placenta, as well, in the following quote.)
Finally, we analyzed ADE of coronavirus entry at different antibody dosages. MERS-CoV entry into cells expressing both viral and Fc receptors demonstrates complex MAb-dosage-dependent patterns. As the concentration of MAb increases, (i) viral entry into DPP4-expressing cells is inhibited more efficiently because MAb binds to the spike and blocks the DPP4-dependent entry pathway, (ii) viral entry into Fc receptor-expressing cells is first enhanced and then inhibited because MAb binds to the Fc receptor to enhance the ADE pathway until the Fc receptor molecules are saturated, and (iii) viral entry into cells expressing both DPP4 and Fc receptor is first inhibited, then enhanced, and finally inhibited again because of the cumulative effects of the previous two patterns. In other words, for viral entry into cells expressing both DPP4 and Fc receptor, there exists a balance between the DPP4-dependent and antibody-dependent entry pathways that can be shifted and determined by MAb dosages. Importantly, ADE occurs only at intermediate MAb dosages. Our study explains an earlier observation that ADE of dengue viruses occurs only at certain concentrations of MAb. While many human tissues express either DPP4 or Fc receptor, a few of them, most notably placenta, express both of them. For other viruses that use viral receptors different from DPP4, there may also be human tissues where the viral receptor and Fc receptor are both expressed. The expression levels of these two receptors in specific tissue cells likely are determinants of MAb dosages at which ADE would occur in these tissues. Other determinants of ADE-enabling MAb dosages may include the binding affinities of the MAb for the viral and Fc receptors. Overall, our study suggests that ADE of viruses depends on antibody dosages, tissue-specific expressions of viral and Fc receptors, and some intrinsic features of the antibody.
THE SPIKE PROTEIN ANTIBODY/Fc RECEPTOR COMPLEX AND SYSTEMIC AUTOIMMUNITY
This then brings us to those who survive the acute infection. Given the previously mentioned paper, everything may be related to LEVELS of antibodies. Could it be that those who “lose” antibodies more quickly post-infection, ironically, fare better in the long run?
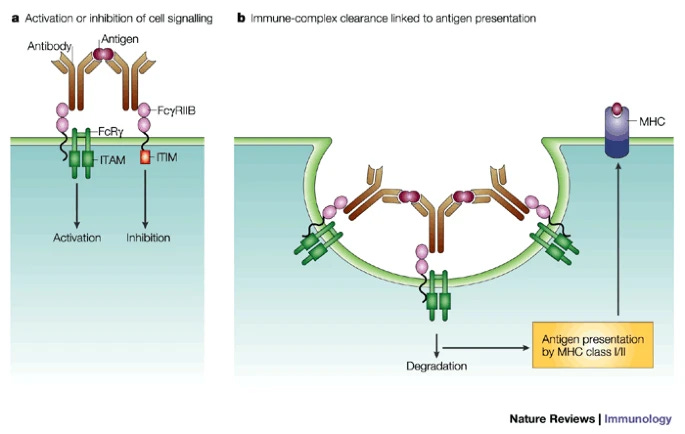
On March 24 of this year, a paper was published in Communications Biology entitled Antibody-dependent enhancement (ADE) of SARS-CoV-2 pseudoviral infection requires FcγRIIB and virus-antibody complex with bivalent interaction.
In this paper they reveal a novel ADE mechanism of SARS-CoV-2 pseudovirus in vitro, FcγRIIB-mediated uptake of SARS-CoV-2/mAb complex with bivalent interaction.
What does this mean?
I believe this is keystone of the systemic autoimmunity we are observing. Based on recent studies of autoimmune diseases in mice, it is activating FcRs which has been shown to promote disease development, whereas the inhibitory FcR FcγRIIB maintains peripheral tolerance. However! This is the VERY RECEPTOR which the COMPLEX INTERACTS WITH!
After all, is not the panoply of Kawasaki disease (MIS-C, MIS-A), dermatomyositis and antineutrophil cytoplasmic antibody (ANCA)-positive vasculitis, systemic lupus erythematosus, polymyositis and catastrophic antiphospholipid syndrome among others what we are observing?
AND! PERHAPS THE MOST FASCINATING POINT! IS IT THE LEVELS OF ANTIBODIES PRESENT WHICH DETERMINE WHO DEVELOPS MIS-C, FOR EXAMPLE? DOES THIS SOLVE THE LONGSTANDING MYSTERY?
I believe it may.
The therapeutic question in all of this is: Could Therapeutic Intravenous Immunoglobulin be an effective therapeutic?
Intravenous immunoglobulin therapy in rheumatic diseases
https://go.gale.com/ps/i.do?p=AONE&u=googlescholar&id=GALE|A258994651&v=2.1&it=r&sid=googleScholar&asid=ea065397
Roles of Fc receptors in autoimmunity
https://www.nature.com/articles/nri856
Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7022351/
Antibody-dependent enhancement (ADE) of SARS-CoV-2 pseudoviral infection requires FcγRIIB and virus-antibody complex with bivalent interaction
https://www.nature.com/articles/s42003-022-03207-0
Antibody-dependent enhancement of SARS coronavirus infection
https://www.hkmj.org/system/files/hkm1603sp4p25.pdf
Bingo Walter! I’ve been waiting for this. I measure SARS-CoV-2 Semi Quant. Total Spike antibodies in all my patients, if possible, and there appears to be a strong correlation between severity of symptoms and disease presentation and level of antibodies.
One of my patients never vaccinated receiving monthly IVIG infusions since at least early 2021 all of a sudden after her December treatment showed very elevated levels of Spike antibodies, in the many thousands where as she did not have higher than 100 previously after community acquired infection. Therefore I suspect that the IVIG supply is contaminated.
Thank you so much!!
Nice finds!
I can help you a bit on this one. I haven't put the diagrams in articles, but have presented them during interviews---the DMED data shows a clear increase in severity of COVID-19 infections among the military (similar age/health profiles with little chance for Simpson's paradoxes). I will put this together in an article and link back here.
Cheers.