
Is the Spike Protein Inducing a Novel, Systemic Necrotic Disease Similar to Brain Radiation Necrosis?
Could Long COVID be this systemic necrotic disease?

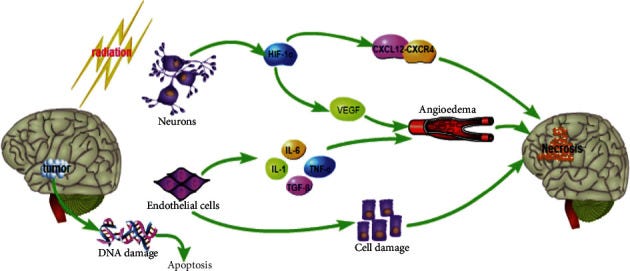
Relevant mechanisms involved in the process of RBN occurrence.
As readers of this Substack may know, I have long compared the damage caused by the Spike Protein to the damage caused by Radiation. I have pursued this concept further. What I have now found is that Long COVID may indeed be a new, systemic necrotic disease. The Spike’s effects on the Endothelium being the genesis of the condition.
After a tremendous amount of searching, I found a model which best describes what I believe the Spike Protein is doing. It is called Brain Radiation Necrosis.
Let’s look at the symptoms of this condition.
Cerebral radiation necrosis is a rare but serious complication of RT (Radiation Therapy). It can occur anywhere from 6 months to years after treatment. It manifests as cell death and edema around the site of the tumor and, depending on the location, can produce discreet neurological deficits and symptoms of increased intracranial pressure, such as headaches. There have been reports of radiation necrosis manifesting as psychiatric symptoms, including depressive symptoms, mood lability, paranoia, delirium, and cognitive impairment.41
Psychiatric Care of the Radiation Oncology Patient
https://www.sciencedirect.com/science/article/pii/S0033318217301123
Now, if we examine the mechanism of Brain Radiation Necrosis, we find that we are in all too familiar territory.
Pathologically, radiation necrosis primarily affects the smaller arterioles and arteries which initially causes coagulative necrosis and then endothelial thickening and infiltration of lymphocytes and macrophages. The inflammation that develops from the infiltration of these immune cells triggers off a whole host of cytokine activity, activation of fibroblasts, and hyalinization of the tissue. Immune-mediated mechanisms that contribute to neurotoxicity have been hypothesized but have not been fully explained.
Hyperbaric Treatment of Brain Radiation Necrosis
https://www.ncbi.nlm.nih.gov/books/NBK431083/#
It all fits, the Spike Protein does the damage that radiation does in BRN. Looking closely, we find evidence that the necrotic phenomena may indeed be systemic. For example, it is a factor in the myopathy of Long COVID.
To further elucidate the pathophysiology of increased muscle weakness, fatigue, and pain after exercise in long COVID patients, we determined whether specific pathological features were present in skeletal muscle before and after the induction of post-exertional malaise. As the biopsy size was variable between participants and time-points, we scored biopsies negative/positive for pathological and immunological parameters. A larger percentage of long COVID patients displayed small atrophic fibers and focal necrosis (Fig. 5A, B), which increased significantly after exercise, indicating an exacerbated tissue damage response in patients with long COVID.
Muscle abnormalities worsen after post-exertional malaise in long COVID
https://www.nature.com/articles/s41467-023-44432-3
Very little research into this explanation for Long COVID has been done, but I am certain more needs to be. What brought me to this point are the parallels to the MHV coronavirus. Necrosis is ubiquitous.
In the MHV-1 mouse model, numerous pathologic changes occur across multiple organ systems during acute infection [4]. In the brain, observed pathologic changes include congested blood vessels, perivascular cavitation, pericellular halos, vacuolation of neuropils, darkly stained nuclei, pyknotic nuclei amid associated vacuolation of the neuropil, and acute eosinophilic necrosis. Cardiac tissue samples display evidence of interstitial edema, vascular congestion, and infiltration of red blood cells between degenerative myocardial fibers. Renal changes consist of tubular epithelial cell degeneration, proximal and distal tubular necrosis, interstitial tissue hemorrhage, and vacuolation of renal tubules. Similarly, liver pathology indicates hepatocyte degeneration, severe periportal hepatocellular necrosis characterized by pyknotic nuclei, congestion, ballooned hepatocytes, vacuolation, piecemeal necrosis, ground glass hepatocytes with voluminous, abundant, granular cytoplasm, as well as peripheral cytoplasmic clearing and central nuclei. During acute infection, apoptotic (acidophil) bodies, abundant inflammatory cells, condensation and dark cytoplasm staining, fatty changes, binucleated hepatocytes, and activated Kupfer cells are also evident.
Furthermore, examination of lung tissue samples obtained from the MHV-1 mouse model reveals severe inflammation, proteinaceous debris filling the alveolar spaces with fibrillar to granular eosinophilic protein strands, the presence of hemosiderin-laden macrophages, peribronchiolar interstitial infiltration, bronchiole epithelial cell necrosis, necrotic cell debris within alveolar lumens, alveolar exudation, hyaline membrane formation, alveolar hemorrhage, and interstitial edema [4]. Notably, the clinical symptoms observed in our MHV-1 mouse model closely mirror the symptomatology identified in patients with the SARS-CoV-2 variants mentioned above [5,6,7].
Furthermore, our MHV-1 mouse model also displayed long-term sequelae affecting multiple organ systems during the 12 months following the initial injection with MHV-1, resembling aspects of long COVID-19 disease observed in humans. Brain tissue samples exhibited severely congested blood vessels, perivascular cavitation, pericellular halos, vacuolation of neuropils, pyknotic nuclei, eosinophilic necrosis, necrotic neurons with fragmented nuclei, and vacuolation. Cardiac tissue samples demonstrated severe interstitial edema, vascular congestion, myocyte necrosis, inflammation, and apoptotic bodies. The kidneys showed tubular epithelial cell degenerative changes, interstitial tissue hemorrhage, vacuolation of renal tubules, inflammation of the renal parenchyma, severe tubular necrosis, and infiltration of macrophages and lymphocytes. Liver samples revealed congestion, ballooned hepatocytes, vacuolation, piecemeal necrosis, and occasional ground glass hepatocytes with voluminous, abundant, granular cytoplasm, central nuclei, and activated Kupffer cells. Additionally, lymphocyte infiltration in sinusoidal spaces, multifocal hepatic necrosis both in the periportal area and near the terminal hepatic veins, increased number of portal veins associated with luminal severe dilatation, activated Kupffer cells with large cytoplasm containing necrotic debris, eosinophilic bodies, mitotic cells, balloon-like liver cells, mild inflammation of the lobular lymphocytic and portal tract, mild hydropic degeneration of liver parenchymal cells, and lipofuscin pigment were also noted.
SPIKENET: An Evidence-Based Therapy for Long COVID
https://pmc.ncbi.nlm.nih.gov/articles/PMC11209161/
If there is any good news in all of this, it is that the condition appears to be treatable and perhaps reversible. This is why we need to examine the necrosis hypothesis as a pathological mechanism of Long COVID. Understanding and lives may be vastly improved.
I will continue to research this mechanism and report to you. Thank you, as always, for your readership, dialogue and support.
...and our government intentionally put it in the mRNA countermeasures and wanted "a shot in every arm". Thank you Walter. May God bless you and guide you. Peace.
Outstanding investigation. I value your work greatly. I am writing an article around your post on Dr Rima Truth Reports substack and recommending your stack.
Keep on doing what you are doing. We all get smarter because of it!