

Friday Hope: Vitamin C and the Extracellular Matrix (ECM)
I propose that Vitamin C may be useful in preventing/treating post-Covid/Spike Protein exposure fibrosis.

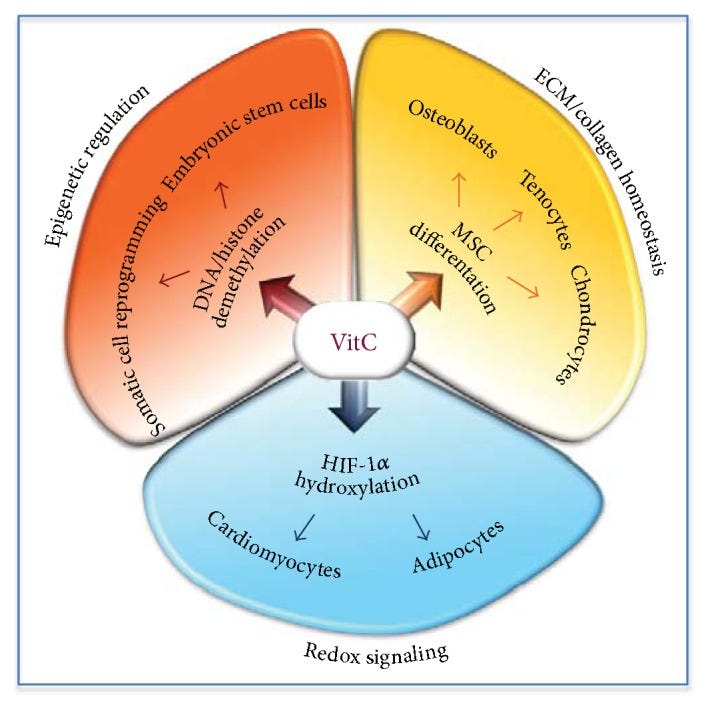
Molecular mechanisms underlying VitC activity on stem cells. VitC-dependent regulation of epigenetic modifications, ECM remodelling and redox balance, control embryonic stem cell self-renewal/proliferation, somatic cell reprogramming, and stem cell differentiation.
One of the most devastating effects of SARS-CoV-2 is that it can induce fibrosis in a significant number of patients as one of its sequelae.
Although mainly it is considered idiopathic, the inflammatory changes in the lungs secondary to the viral infection can lead to fibrotic changes. This can be more likely with ARDS than pneumonia due to the diffuse alveolar damage and resultant type II pneumocyte hyperplasia [3]. Pulmonary fibrosis is characterized by the lungs’ inability to reconstruct the damaged alveolar epithelium, persistence of fibroblasts, and excessive deposition of collagen and other extracellular matrices (ECM) components. This is accompanied by the destruction and alteration of normal lung architecture [12].
Post-COVID-19 fibrosis is one of the emerging complications of COVID-19 pneumonia and ARDS. It is estimated to be prevalent in around one-third of COVID-19 infected hospitalized patients. More extensive studies are needed to investigate this occurrence and test the efficacy of already tested drugs (for idiopathic pulmonary fibrosis) such as antifibrotics for post−COVID-19 fibrosis. We suggest doing a 6-minute walk test to assess exertional desaturation in patients who are fulfilling other discharge criteria for COVID-19 pneumonia and ARDS.
Post COVID-19 fibrosis, an emerging complication of SARS-CoV-2 infection
https://www.sciencedirect.com/science/article/pii/S2214250920303498
In terms of inducing fibrosis, one may observe a direct parallel of the effects of the Spike Protein with Paraquat exposure. Vitamin C has proven effective in treating the induced fibrosis of Paraquat. Of course, trials are needed, but given the similarity of mechanisms, it is highly likely that Vitamin C will have a similar effect on Spike Protein induced fibrosis.
Paraquat (PQ) is one of the most widely employed herbicides that is used worldwide and it causes severe toxic effects in humans and animals. A PQ exposition can lead to pulmonary fibrosis (PF) and the mechanisms seem to be linked to oxidative stress, although other pathways have been suggested. Antioxidants can be useful as a therapy, although interventions with this kind of system are still controversial. Hence, this study has investigated the role of ascorbic acid (vitamin C) post-treatment on PQ-induced PF in male C57/BL6 mice. Pulmonary fibrosis was induced by a single PQ injection (10mg/kg; i.p.). The control group received a PQ vehicle. Seven days after the PQ or vehicle injections, the mice received vitamin C (150 mg/kg, ip, once a day) or the vehicle, over the following 7 days. Twenty-four hours after the last dose of vitamin C or the vehicle, the mice were euthanized and their bronchoalveolar lavage fluid (BALF) and their lungs were collected. The data obtained showed that vitamin C reduced the cellular recruitment, the secretion of IL-17 –a cytokine involved in neutrophils migration, TGF-β–a pro-fibrotic mediator and the collagen deposition.
Beneficial effects of ascorbic acid to treat lung fibrosis induced by paraquat
https://pmc.ncbi.nlm.nih.gov/articles/PMC6218022/
This benefit may extend beyond induced pulmonary fibrosis, as Vitamin C in combination with Vitamin E has been shown to reduce fibrosis in NASH.
Results
Forty-five patients completed 6 months of therapy without significant side effects. Vitamin treatment resulted in a statistically significant improvement in fibrosis score (p = 0.002). No changes were noted in inflammation with treatment.
Conclusions
Vitamin E and vitamin C, in the doses used in this study, were well tolerated and were effective in improving fibrosis scores in NASH patients. No improvement in necroinflammatory activity or ALT was seen with this combination of drug therapy. A larger, multicenter, longer-term trial with vitamin E and vitamin C seems to be warranted.
Vitamin E and vitamin C treatment improves fibrosis in patients with nonalcoholic steatohepatitis
https://www.sciencedirect.com/science/article/abs/pii/S0002927003017866
There is, of course, evidence that Vitamin C has proven beneficial in preventing and treating acute COVID infection, we well.
In summary, vitamin C possesses positive impacts on curing of infection and this may play a protective role in the current COVID-19 pandemic through boosting the immune system. Because of its antioxidant and anti-inflammatory properties, vitamin C is widely used in the treatment of a variety of diseases. Vitamin C functions as a powerful antioxidant, assisting in normal neutrophil function, scavenging ROS, regenerating vitamin E, modulating signaling pathways, activating pro-inflammatory transcription factors, activating the signaling cascade, nuclear factor B (NFB), regulating inflammatory mediators, gene regulation, phagocytosis, and signaling pathways in T cells, and increasing neutrophil motility to the site of infection. So, to develop strong immunity against COVID-19 infection, a regular administration of vitamin C is required.
Interesting results have been obtained by administering larger doses of IV Ascorbic acid to COVID-19 infected patients in China and the United States. Whether vitamin C may assist specifically in treating COVID-19 individuals who are elderly, have fundamental illnesses, or are members of African American populations, it would be interesting to see if this can be shown. Briefly summarised, high-dose vitamin C has been shown to reduce inflammation, improve oxygen support status, and reduce mortality in COVID-19 patients, all without causing any negative side effects. Additionally, it may be beneficial for specific subgroups of patients with severe and critical condition, as well as for older individuals. High-dose vitamin C may prove to be an effective treatment for COVID-19. Furthermore, there is an urgent need to investigate the direct relationship between serum/plasma nutritional C levels and the incidence and severity of COVID-19 infection.
Role of vitamin C in preventing of COVID-19 infection, progression and severity
https://pmc.ncbi.nlm.nih.gov/articles/PMC8995185/
It would be very interesting to know the data of serum Vitamin C levels correlated with COVID infection rates, acute COVID severity/duration and development of Long COVID. We have much to learn. However, given the evidence showing Vitamin C’s therapeutic effects on fibrosis, I ask clinicians to evaluate these benefits and treat accordingly.
I am ever thankful for your financial support, dialogue and readership. Finding ways to counteract the Spike Protein gives me hope that we may, eventually, be able to keep this pathogenic protein at bay. Blessings, joy and peace for now, the upcoming weekend, and always.
I understand that the best form of vitamin C is that which contains both ascorbic acid _and_ the often overlooked bioflavonoids. Vitamin C with rose hips is a better form of vitamin C for one example. The effect is synergistic, not just additive.
As for vitamin E, there are eight forms. The most common (and also cheapest) only contain one of these eight forms. It may be better to get a complete vitamin E.
And as long as we're on the subject of vitamins, if you are taking vitamin D3, it is probably best to pair it with vitamin K2. Vitamin D3 has the effect of increasing the absorption of calcium in the gut by a huge factor, but it goes everywhere, including the soft tissues and arteries. Vitamin K2 is believed to finish the job in a better way by encouraging the calcium to head for the bones as it should.
Anyone with gum disease should take vitamin C---ascorbic acid and rose hips--to strengthen the endothelium in the mucosa throughout the system.