
Friday Hope: Signaling Pathway Inhibitors: If it Acts Like Cancer, Treat it Like Cancer
Friday Hope: Signaling Pathway Inhibitors: If it Acts Like Cancer, Treat it Like Cancer
Signaling Pathway Inhibitors (SPIs) may be a powerful way to stop pathogenic processes of the Spike before they start.

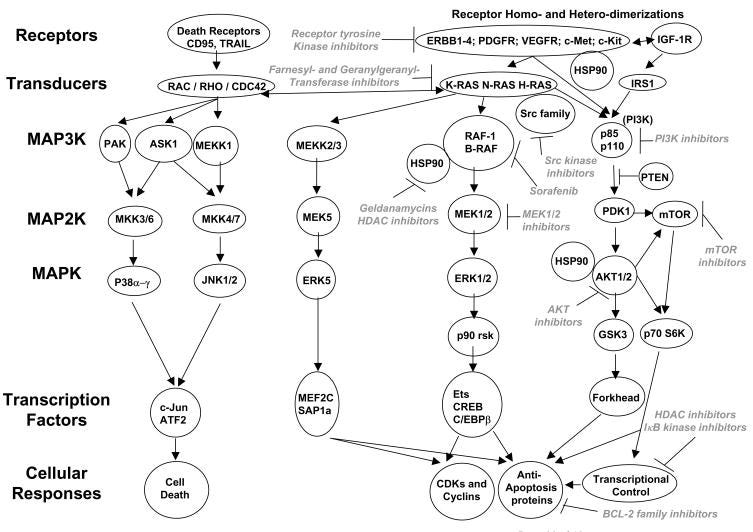
If we look at the signaling induced by the Spike Protein, we find that it perfectly mimics the signaling induced by cancer cells:
Cancer cells have elevated activities within multiple signal transduction pathways due to (reviewed in Valerie et al., 2007; Dent et al, 2003):
- the increased expression of paracrine ligands acting on growth factor receptors;
- receptor over-expression;
- oncogenic activating mutations of receptors and downstream RAS GTP binding proteins;
- inactivation of tumor suppressor lipid and protein phosphatases;
- oncogenic activation of downstream protein and lipid kinase
Therefore, it makes sense that we should try inhibiting these very same pathways while the body is exposed to the Spike Protein. By doing so, we may prevent many, if not all of the pathogenic effects of the Spike. This treatment protocol could prevent the development of Long COVID and perhaps treat or cure those who currently have Long COVID.
The Spike Protein also activates pathways similar to those activated by cancer treatment.
Cancer cells contain multiple signal transduction pathways whose activities are frequently elevated due to their transformation, and that are often activated following exposure to established cytotoxic therapies including ionizing radiation and chemical DNA damaging agents. Many pathways activated in response to transformation or toxic stresses promote cell growth and invasion and counteract the processes of cell death.

Therapeutic drugs that target the cell cycle
Kinase inhibitors that modulate the cell cycle have frequently been combined with toxic drugs and/or radiation which cause DNA damage. This will lead to inappropriate cell cycle progression with damage DNA and result in tumor cell death. Inhibition of PARP1 ADP ribosylation activity suppresses the ability of DNA damage to activate ATM/ATR as well as increase DNA repair processes.
Perhaps the greatest takeaway from studying SPIs and cancer is finding therapies that suppress the ability of DNA damage to activate ATM/ATR as well as increase DNA repair processes.
It is through a combination of agents, similar to those used in cancer treatment, that we may be able to prevent severe COVID disease, prevent Long COVID and treat those currently with Long COVID.
There are profound levels of survival signaling redundancy and of signaling plasticity which permit tumor cells to adapt and overcome multiple environmental and therapeutic stresses. Collectively this implies that the use of highly specific targeted therapies, often using single inhibitory agents as was initially employed with ERBB1 inhibitors, was almost guaranteed to fail. In a few specific tumor cell types, the single agent cytotoxicity of a kinase inhibitor is evident due to very specific oncogene addiction of those cells. However, many of the most promising signal transduction modulatory drug combinations involve agents that both act to suppress survival signaling within multiple pathways and act to suppress expression of multiple apoptosis inhibitory proteins. Thus agents that inhibit mTOR and suppress expression of many proteins; those that destabilize multiple activated signaling proteins through HSP90 inhibition; those that block Cdk9 (p-TEFb) function and suppress expression of multiple proteins and those that inhibit multiple receptor tyrosine kinases appear to represent the best avenues for therapeutic efficacy in multiple malignancies.
The following, from the paper I based this post on, may be a very good place to start:
Clinically relevant combinations of therapeutic drugs: pre-clinical and clinical testing
Below is a short list of some of the published/tested combinations of novel cancer therapeutic drugs.
Growth factor Receptor Tyrosine Kinases
ERBB1–4 family inhibitors + mTOR inhibitors
ERBB1–4 family inhibitors + c-Met inhibitors
ERBB1–4 family inhibitors + IGF1R inhibitors
ERBB1–4 family inhibitors + Vascular Endothelial Growth Factor Receptor family inhibitors
PDGFR/VEGFR/FLT3 inhibitors + mTOR inhibitors
Non-receptor Tyrosine Kinases
Abl kinase inhibitors + Src family tyrosine kinase inhibitors
Tyrosine kinase inhibition(s) + Inhibition of proteasome degradative activity
Small GTPase Inhibitors
Ras family farnesylation/geranylgeranylation inhibitors + Checkpoint/Chk1 regulatory kinase inhibitors
Intracellular signal transduction intermediates
Phosphatidyl inositol 3 kinase inhibitors + MEK1/2 inhibitors
Phosphatidyl inositol 3 kinase inhibitors + mTOR inhibitors
AKT inhibitors + mTOR inhibitors
Inhibitors of heat shock protein 90 + MEK1/2 inhibitors
Regulation of Transcription
Histone deacetylase inhibitors + Sorafenib
Inhibition of proteasome degradative activity + Histone deacetylase inhibitors
IKK inhibitors + Histone deacetylase inhibitors
Inhibition of proteasome degradative activity + Cyclin dependent kinase inhibitors
Regulation of cell cycle progression and genomic stability
Cyclin dependent kinase inhibitors + Histone deacetylase inhibitors
Checkpoint/Chk1 regulatory kinase inhibitors + MEK1/2 inhibitors
Inhibitors of heat shock protein 90 + Cyclin dependent kinase inhibitors
Cyclin dependent kinase inhibitors + Phosphatidyl inositol 3 kinase inhibitors
Regulation of mitochondrial function
Bcl-2 family protein inhibitors + Inhibition of proteasome degradative activity
Synergistic combinations of signaling pathway inhibitors: Mechanisms for improved cancer therapy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696566/
By commencing trials using the above combinations of agents in those with COVID disease, Long COVID and those exposed to the Spike Protein or SARS-CoV-2 we may be able to hone an extremely effective Spike Protein/SARS-CoV-2 treatment protocol.
I love your efforts to contribute to the cure and treatment for the damage this virus and "vaccine"-not a- vaccine has done. Your writing is far above my pay grade, but having read so much about the topic over the last 3 years, I can now understand some of it. Thank You.
Of course authorities, hospitals and doctors would have to acknowledge that the spike is toxic and can cause cancers - or cancer-like problems - before treatment could commence, and I doubt they'll do that. It would be an admission of the inherrent dangers of the Covid 'vaccines' as well as probably casting doubt on the mRNA platform itself, the use of which is only in it's infancy. Everything under the sun will be reformulated into cheaper, faster, mRNA 'vaccines' and drugs, the shitshow is sadly only beginning