
Friday Hope: Cetylpyridinium Chloride: Common Mouthwash Strongly Inhibits SARS-CoV-2 and its Spike Protein
Friday Hope: Cetylpyridinium Chloride: Common Mouthwash Strongly Inhibits SARS-CoV-2 and its Spike Protein
Using mouthwash before leaving the house or having company over may block infection by SARS-CoV-2 and its Spike Protein.

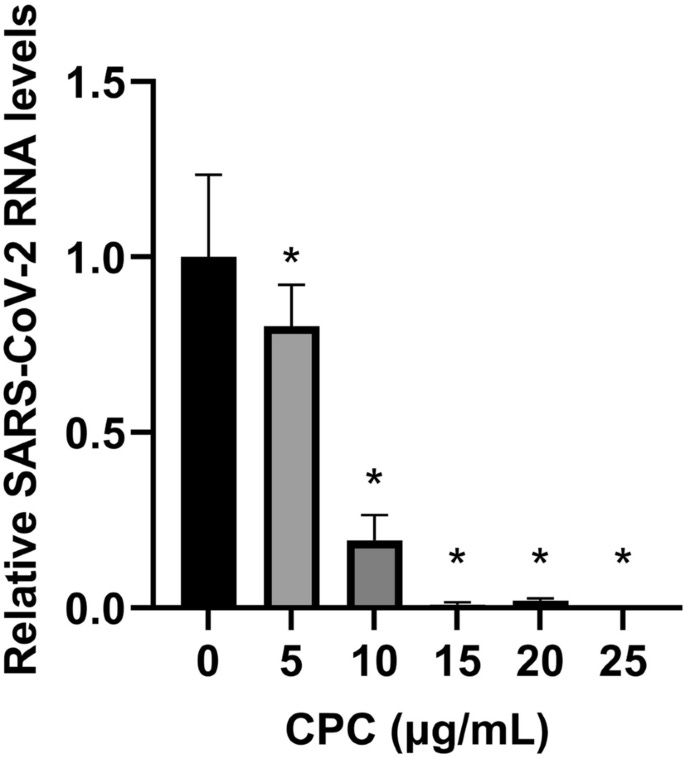
Antiviral efficacy of CPC against SARS-CoV-2 by qRT-PCR. VeroE6/TMPRSS2 cells were inoculated with SARS-CoV-2 Wuhan strain at a multiplicity of infection (MOI) of 0.01 after mixing equal amount CPC. At 24 h postinfection, the relative levels of viral N protein RNA were evaluated quantitatively by qRT-PCR. (*p < 0.05).
Given that, over the years, the absolute best way to deal with the Spike Protein is to block it from the start, I have placed a primary importance on treating everything Spike related as pathologies of Access. Deny access, remove all threats. The authorities take a different view: Grant access, stomp it out. So, as all of us know, the medical authorities therefore appealed to us (read forced) to take a gene therapy to “help” our bodies fight off the novel (read created) virus SARS-CoV-2.
Had those same authorities looked to the dental hygiene aisle of the local supermarket instead of unproven mRNA “therapies,” they would have actually found something safe and effective against the virus and its Spike Protein.
MOUTHWASH!
Researchers at Hokkaido University in Sapporo, Japan looked into the compound Cetylpyridinium Chloride (CC), which is the active ingredient of such mouthwash products as Crest Pro-Health Intense. What they discovered was remarkable. Even at concentrations lower than most mouthwash products, CC was quite effective at disrupting SARS-CoV-2.
Cetylpyridinium chloride (CPC), a quaternary ammonium compound, which is present in mouthwash, is effective against bacteria, fungi, and enveloped viruses. This study was conducted to explore the antiviral effect of CPC on SARS-CoV-2. There are few reports on the effect of CPC against wild-type SARS-CoV-2 at low concentrations such as 0.001%–0.005% (10–50 µg/mL). Interestingly, we found that low concentrations of CPC suppressed the infectivity of human isolated SARS-CoV-2 strains (Wuhan, Alpha, Beta, and Gamma) even in saliva. Furthermore, we demonstrated that CPC shows anti-SARS-CoV-2 effects without disrupting the virus envelope, using sucrose density analysis and electron microscopic examination. In conclusion, this study provided experimental evidence that CPC may inhibit SARS-CoV-2 infection even at lower concentrations.
Upon examination, CC inhibited the infectivity of all strains it had available at the time of the study.
We have examined the SARS-CoV-2 strains, including Wuhan, Alpha, Beta, and Gamma, which belong to VOC. The plaque assay demonstrated that CPC significantly suppressed the infectivity of all examined SARS-CoV-2 directly in a dose-dependent manner (Figs. 1a–d, S1). CPC (50 μg/mL) treatment completely inactivated SARS-CoV-2 Wuhan strain similarly as Triton X-100 (1%).
The conclusion of the study is obvious.
The use of CPC-containing products may lead to a reduction in the number of newly infected covid patients. Additionally, it may be a means of preventive measures in poorly vaccinated countries. We anticipate that CPC will be used as one of the tools to prevent the onset and infection of SARS-CoV-2.
Antiviral effect of cetylpyridinium chloride in mouthwash on SARS-CoV-2
https://www.nature.com/articles/s41598-022-18367-6
Even for those who do become infected, using CC mouthwash may also attenuate the severity of COVID disease. A review of CC randomized controlled trials found that, due to reduced viral load, those with COVID disease could reduce its transmissibility and severity.
Results
Six studies with a total of 301 patients that met the inclusion criteria were included. The studies reported the efficacy of cetylpyridinium chloride mouthwashes in reduction on SARS-CoV-2 salivary viral load compared to placebo and other mouthwash ingredients.
Conclusion
Mouthwashes containing cetylpyridinium chloride are effective against salivary viral load of SARS-CoV-2 in vivo. There is also the possibility that the use of mouthwash containing cetylpyridinium chloride in SARS-CoV-2 positive subjects could reduce transmissibility and severity of COVID-19.
Efficacy of Cetylpyridinium Chloride mouthwash against SARS-CoV-2: A systematic review of randomized controlled trials
https://onlinelibrary.wiley.com/doi/full/10.1111/omi.12408
Yet another paper demonstrated similar efficacy for chlorhexidine gluconate (CHG), Listerine, Colgate Peroxyl and povidone-iodine.
A 5% (v/v) dilution of Colgate Peroxyl or povidone-iodine completely blocked viral infectivity. A similar 5% (v/v) dilution of Listerine or CHG had a moderate suppressive effect on the virus, but a 50% (v/v) dilution of Listerine or CHG blocked viral infectivity completely. Mouth rinses inactivated the virus without prolonged incubation. The new infectivity assay, with limited impacts of mouth rinse-associated cytotoxicity, showed the differential effects of mouth rinses on SARS-CoV-2 infection. Our results indicate that mouth rinses can significantly reduce virus infectivity, suggesting a potential benefit for reducing SARS-CoV-2 spread.
Differential Effects of Antiseptic Mouth Rinses on SARS-CoV-2 Infectivity In Vitro
https://www.mdpi.com/2076-0817/10/3/272
I wish everyone a minty-fresh Spring weekend! As we continue to learn, we continue to assemble a tool kit which will help us protect our bodies from the invasion and pathogenic effects of SARS-CoV-2 and its Spike Protein.
We heard about Cetylpyridinium Chloride in mouthwash in 2020. I have been using it since then. I particularly rinse after returning home when I have had to mingle with people at stores. We use Colgate Total. I had not heard of using povidone-iodine before and wasn't aware it could be taken internally like Nascent Iodine ( my wife was using it = 6 drops in water to treat something else but she was extremely hard of hearing and her hearing came back and has stayed good). Would love to know how to use the povidone-iodine and what dosing.
This stuff can really stain your teeth and I suspect it is far more toxic than they indicate (which is still significant). Why not stick with hydrogen peroxide?