

Friday Hope: Back to Basics: Diet and Exercise Improve COVID Outcomes
A new paper confirms one of my early (2021) publications and provides concrete recommendations.

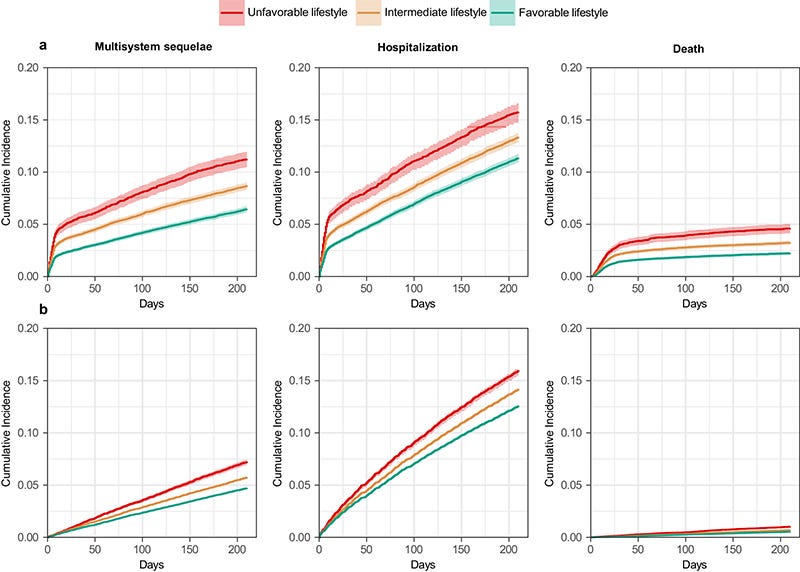
Cumulative incidence curves of composite multisystem sequelae, death, and hospitalization among participants with and without SARS-CoV-2 infection.
a Participants with SARS-CoV-2 infection. b Participants with no evidence of SARS-CoV-2 infection. Outcomes were ascertained 0–210 days after SARS-CoV-2 infection. Event rates are presented for the unfavorable lifestyle category (red), the intermediate lifestyle category (orange), and the favorable lifestyle category (green). The shadow of cumulative incidence curves represents 95% CIs.
Let me tell you a story. This will give you a glimpse into how I conduct research and how I determine what to research. It will also give us hope as it reveals a well thought out and researched therapeutic yields beneficial results.
It is the summer of 2020. The Pandemic is in full swing. We see severe COVID and deaths everywhere. Everywhere except Africa, that is. This was known at the time as “The African paradox.”
Since COVID-19 became a pandemic, projection models were developed for Africa, with the assumption that SARS-CoV-2 has an exponential pattern of transmission. Crowded social life and poor personal hygiene in Africa can be conducive for COVID-19 spread. However, as of July 20, 2020, only about 9691 COVID-19 deaths have been reported from African continent among a population of 1.34 billion (compared to 143 000/328.2 million in the US alone). Although the number of infected subjects increased considerably during mid-July 2020 reaching about 597223 confirmed cases, the case fatality remained remarkably low in Africa.
COVID-19 pandemic: The African paradox
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7506193/
Researchers and physicians were perplexed. Why was Africa spared? What is it that seemingly protects them? While the world was perplexed, I was not. Due to the fact that my other area of research interest is Obesity, I immediately knew the answer: Diet. And in particular, Sugar and the Western diet/sedentary lifestyle. I knew it, but I had to prove it.
So began the research. Diving into hard to find and difficult to assemble statistics. I persevered and found the evidence. Statistics on sugar consumption for virtually every nation. Statistics on calories consumed. Statistics on physical activity. I assembled all this data, and, when put together, was exactly the evidence I expected to find.
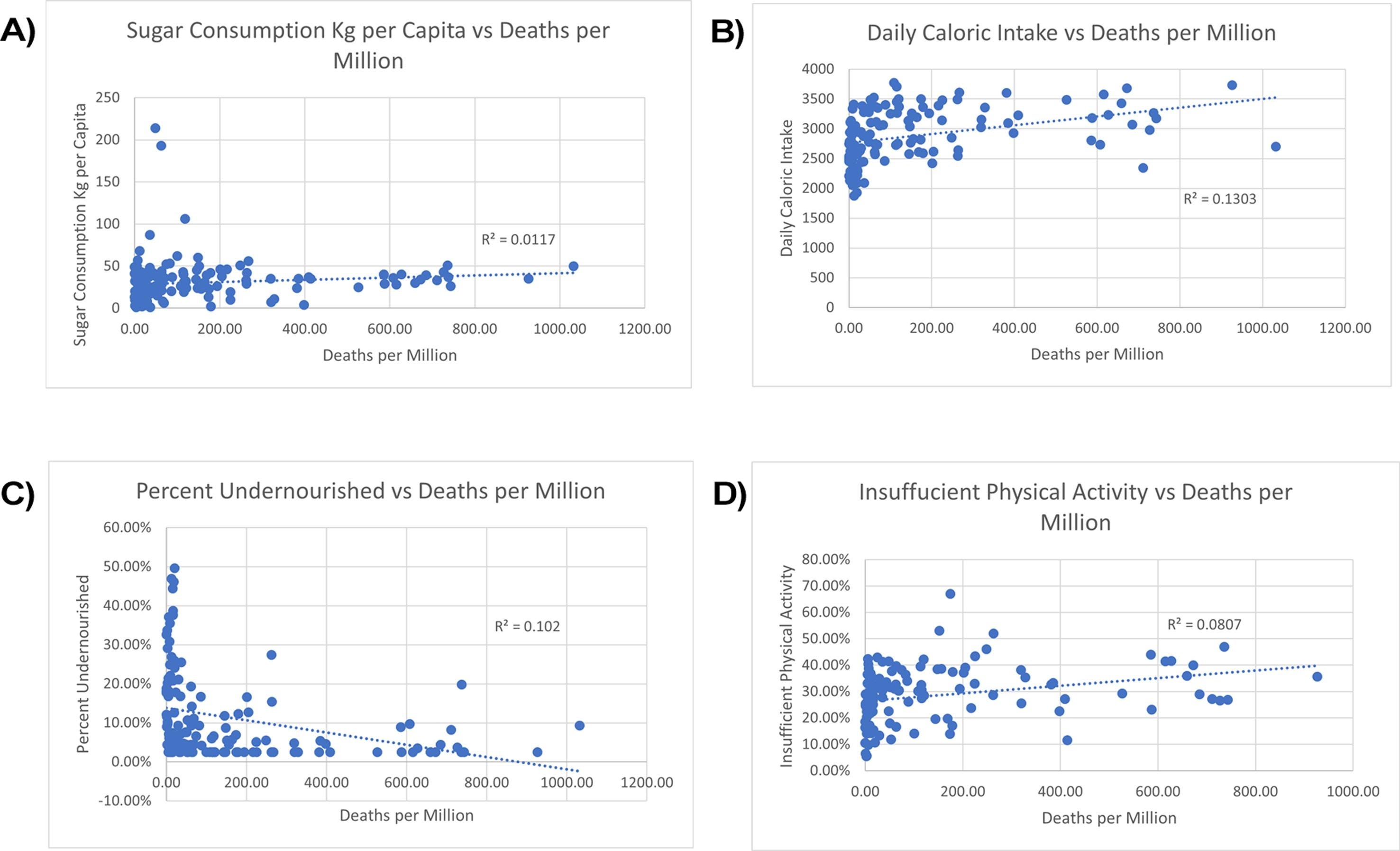
There is a marked difference is COVID-19 mortality globally. In Western and Central Africa, death rates are remarkedly low. For example, the death rates in Niger and Chad are 2.85 per million and 5.84 per million, respectively [1], contrasting to death rates of 677.27 per million for the USA and 662.85 per million for the UK [1], [12]. The numbers from Western and Central Africa, are unexpected, because of local challenges in healthcare and PPE, one of the explanations could be a more active lifestyle and healthier diet. Individuals on a typical Western diet consume copious amounts of sugar but do not expend the energy the excess sugar provides. Due to increased sugar consumption and a lack of physical activity, these individuals are prone to obesity and Type 2 Diabetes Mellitus (DM), which are associated with insulin resistance and impaired glucose metabolism [13]. Fig. 1a shows a general trend between national sugar consumption per capita and COVID-19 mortality rates [1], [14]. Countries with low rates of sugar consumption per capita, like Niger at 1 Kg and Chad at 2 Kg, have low mortality rates of 2.85 and 5.84 per million, respectively. In contrast, countries with high rates of sugar consumption per capita such as the Russian Federation at 42 Kg and Israel at 56 Kg have high mortality rates of 178.5 and 267.34 per million, respectively. An exception to this trend is Singapore; despite a high rate of sugar consumption per capita at 46 Kg, the country has a remarkedly low mortality rate of 4.79 per million. One possible explanation is that Singapore has instituted strict lockdown policies and excellent testing and contact tracing efforts, which have proven effective in halting the spread of SARS-CoV-2 [15]. Fig. 1b shows trend between daily caloric intake per capita and mortality rates [1], [16]. Countries with low national averages for daily caloric intake generally have lower death rates than countries with high averages. For example, the Central African Republic and Uganda have low national averages for daily caloric intake at 1879 and 2130, respectively, and have low mortality rates of 12.85 and 2.16 per million, respectively. In contrast, the United States and Belgium report national averages of 3682 and 3733 calories per day, respectively, and have high mortality rates of 672.22 and 926.43 per million, respectively. Fig. 1c shows that calorie restriction plays a role in reducing COVID-19 severity, as seen in undernourished individuals [1], [16]. Using data from the countries just mentioned, the Central African Republic and Uganda each have an undernourished population of 46.9% and 33.7%, respectively. The United States and Belgium each have only 2.5% of their population undernourished. Lastly, Fig. 1d shows a trend between a lack of physical activity and severe COVID-19 symptoms and mortality [1], [17]. Countries with low rates of insufficient physical activity, such as the Central African Republic and Uganda, which report 14.3% and 5.5% of their respective populations not meeting the daily requirements for sufficient physical activity, have low death rates as mentioned above. In contrast, countries that have a high percentage of their population that does not meet the daily requirements for sufficient physical activity have high death rates. For example, 40% and 35.7% of the populations in the United States and Belgium, respectively, do not meet the daily requirements for sufficient physical activity. For certain countries, there was a strong correlation between multiple factors analyzed. For example, Belgium has a high per capita death rate of 926.43 per million, a high daily caloric intake rate of 3733 calories, a high percentage of the population that does not get the recommended amount of exercise (35.7%) and a high annual consumption rate of sugar (35 Kg per capita). Other countries, such as China, which has a high caloric intake per capita (3108) yet have a very active public, with only 14.1% of sedentary population. China has a low death rate of 3.23 per million. These observations are in accord with Horton’s point that “Syndemics are characterized by biological and social interactions between conditions and states, interactions that increase a person’s susceptibility to harm or worsen their health outcomes.”
Could diet and exercise reduce risk of COVID-19 syndemic?
https://www.sciencedirect.com/science/article/pii/S0306987721000207
So, “The African paradox,” at least to me, wasn’t a paradox at all.
Here we are some four years later, and we now have concrete proof that my hypothesis was correct. In a paper published last week we discover:
Effective prevention strategies for post-COVID complications are crucial for patients, clinicians, and policy makers to mitigate their cumulative burden. This study evaluated the association of modifiable lifestyle factors (smoking, alcohol intake, BMI, physical activity, sedentary time, sleep duration, and dietary habits) with COVID-19 multisystem sequelae, death, and hospitalization in the UK Biobank cohort (n = 68,896). A favorable lifestyle (6-10 healthy factors; 46.4%) was associated with a 36% lower risk of multisystem sequelae (HR, 0.64; 95% CI, 0.58-0.69; ARR at 210 days, 7.08%; 95% CI, 5.98-8.09) compared to an unfavorable lifestyle (0-4 factors; 12.3%). Risk reductions spanned all 10 organ systems, including cardiovascular, coagulation, metabolic, gastrointestinal, kidney, mental health, musculoskeletal, respiratory disorders, and fatigue. This beneficial effect was largely attributable to direct lifestyle impacts independent of corresponding pre-infection comorbidities (71% for any sequelae). A favorable lifestyle was also related to the risk of post-COVID death (HR 0.59, 0.52-0.66) and hospitalization (HR 0.78, 0.73-0.84). These associations persisted across acute and post-acute infection phases, irrespective of hospitalization status, vaccination, or SARS-CoV-2 variant. These findings underscore the clinical and public health importance of adhering to a healthy lifestyle in mitigating long-term COVID-19 adverse impacts and enhancing future pandemic preparedness.
Also, please note that the associations are IRRESPECTIVE OF VACCINATION. I believe this point is crucial.
The good news for us today, is that we have specific, concrete recommendations as to what those healthy living guidelines are to protect us from COVID, and to a certain degree, the Spike Protein. Here they are:
< or = to four drinks per week.
≥150 min/week moderate or ≥ 75 min/week vigorous of physical activity.
≥ 400 g/day fruit and vegetable intake.
< 4 h/day sedentary time.
7-9 h/day sleep.
≥1 portion/week oily fish.
≤3 portion/week red meat.
≤1 portion/week processed meat.
Modifiable lifestyle factors and the risk of post-COVID-19 multisystem sequelae, hospitalization, and death
https://www.nature.com/articles/s41467-024-50495-7#Sec18
Of course, these are great guidelines to follow in times of sickness and in health. However, it is especially important to follow these guidelines if you are sick with COVID and almost certainly if you are suffering from Spike Protein injury/pathology. Please remember this is a work of medical research and not medical advice. Please consult with your Primary Care Provider before beginning any dietary, exercise or lifestyle regimen.
I would like to take a moment to thank everyone who has Subscribed and/or Donated during this year’s Annual Appeal. Eleven subscribers became Paid Subscribers and we now have a total of 350 Paid Subscribers. Thank you! As I state every week, I am an independent researcher and not on the payroll of any institution. But I am aboslutely OK with that. We are our institution, and I am beholden to no overseers telling me what I may and may not research and publish.
I wish all a blessed, healthy and joyous summer weekend.
Walter, one more biggie, eliminate all industrial vegetable seed oils form the diet.
This is why I dropped seventy pounds and I eat no sugar or processed foods. No seed oil. Took me over a month to detox, but it was worth. I’m ready for the next round. Not jabbed. I refused.