

ARE COVID AND LONG-COVID COMPLETELY A B-CELL MEDIATED AUTOIMMUNE DISEASE? IS INNATE IMMUNITY THE ONLY TRUE DEFENSE? AND IS INNATE IMMUNITY DIMINISHED WITH EACH EXPOSURE TO THE SPIKE PROTEIN?
The Self-Immolation of Severe COVID - More Very Disturbing SARS Research from 2005


Building on yesterday’s post.
AGAIN, A BIT OF HISTORY
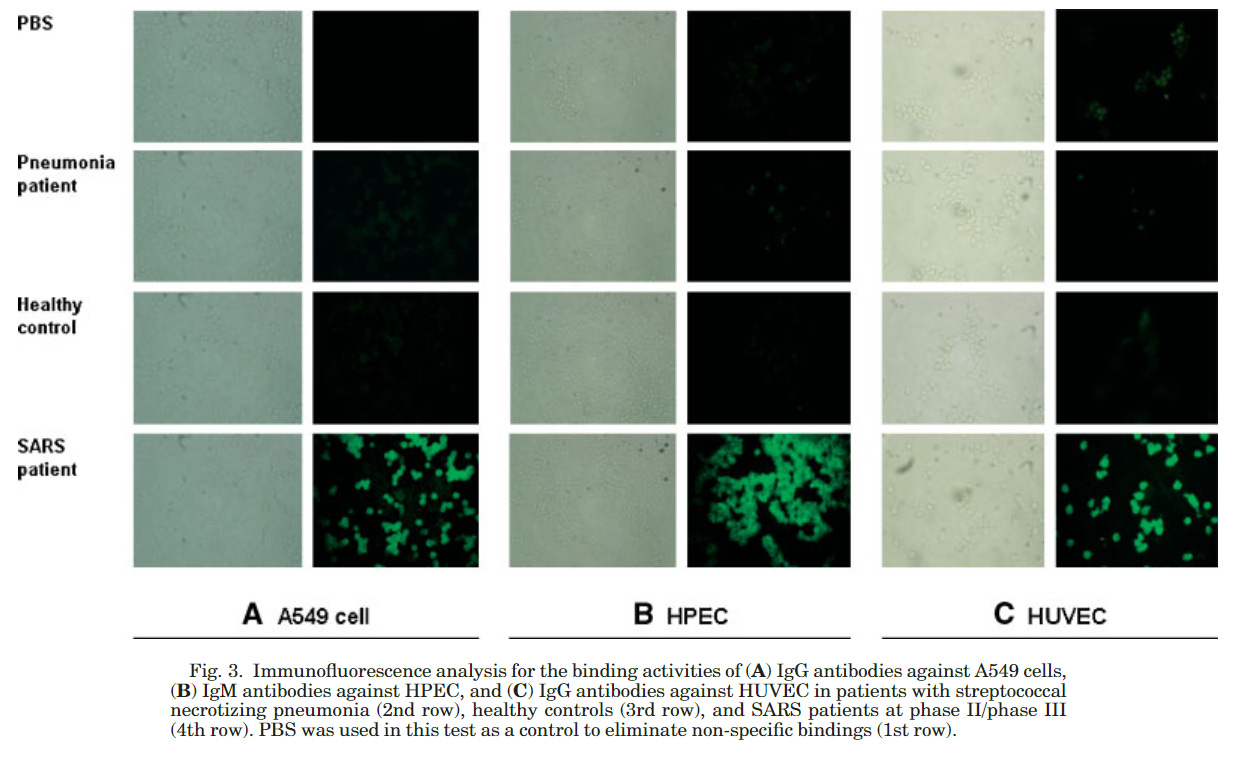
Imagine my surprise when I read this paper from 2005 (yes, you read that correctly, 2005) - Autoantibodies Against Human Epithelial Cells and Endothelial Cells After Severe Acute Respiratory Syndrome (SARS)-Associated Coronavirus Infection
The conclusion is nothing short of absolutely shocking:
In summary, although more studies should be designed and performed to identify the disease-specific autoantigens, the presence of AEpCA and AECA after SARS-CoV infection may represent the severe pulmonary injury and vascular damage in these SARS patients. These autoantibodies also seem to have the potential to damage some epithelial cells and endothelial cells, and these reactions provide another immunological clue fora better understanding of the pathogenesis of SARS. Because of the possible pathogenic potential of these autoantibodies, it is suggested to exclude the possibility of cross-reactions to these primary cells in the development of SARS vaccine.
I now believe that this induction of autoimmunity is the cause of Severe COVID, Fatal COVID and, ultimately, Long COVID.
AN IMPORTANT ASPECT OF THE INNATE IMMUNE RESPONSE
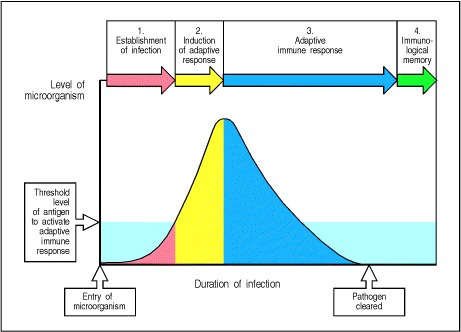
If the innate immune system is able to quickly clear a pathogen, then an adaptive immune response is not needed to combat the infection. Therefore no antibodies are employed against the pathogen. However, adaptive immunity is triggered when an infection eludes the innate defense mechanisms and generates a THRESHOLD DOSE OF ANTIGEN. This antigen then initiates an adaptive immune response, which becomes effective only after several days, the time required for antigen- specific T cells and B cells to locate their specific foreign antigen, to proliferate, and to differentiate into armed effector cells.
I believe it is this very activation of the adaptive immune system which is causing severe COVID, fatal COVID and Long COVID. This is also why a vast majority of those infected have little to no symptoms. Their innate immune system clears the virus and the adaptive immune system does not become involved.
Yet, it appears that the Spike Protein itself “wants” to ensure that the adaptive immune response is employed. The protein suppresses ACE2 and Type I Interferon expression. Furthermore, there has been evidence presented that vaccination induces a profound impairment in type I interferon signaling.
Do you understand the implications? If the innate immune system is impaired and cannot clear the virus, then the adaptive immune system is activated, setting in motion the potential creation of autoantibodies.
If we look at the autoimmune conditions appearing, including MIS-C and MIS-A we must note the following from Characterization of autoantibodies to endothelial cells in systemic sclerosis (SSc): association with pulmonary fibrosis.
AECA (anti-endothelial cell antibodies) were also detected in Kawasaki disease, systemic vasculitis, multiple sclerosis, Wegener's granulomatosis, and Takayasu arteritis.
I am not the only one to raise these concerns. A Letter to the Editor from May of last year was titled Anti-Endothelial Cell Antibodies are not frequently elevated in hospitalized patients with COVID-19.
In it, the authors express their concerns over the title’s implications, questioning them.
While the presence of AECA may represent an epiphenomenon of endothelial dam-age, there is a possibility that pathogenic AECA could be driving the vasculopathy in COVID-19.
The conclusion is very telling:
In conclusion, AECA identification was a relatively infrequent finding in COVID-19 patients on admission, and their presence, albeit in only 2/33 patients, was not associated with disease severity. However, as the autoantibodies were only measured at admission, we cannot exclude the possibility of pathogenic AECA developing later in the course of disease.
I don’t need to tell you where I stand on that possibility.
So, ultimately, what are we looking at? I refer you to yesterday’s post for the mechanism of these autoantibodies appearance. We must also consider Molecular Mimicry contributing to the development of the autoantibodies.
SUDDEN DEATHS
I would like to conclude this post with the suggestion that, indeed, the autoantibodies generated by the presence of the Spike Protein may indeed be responsible for the deluge of sudden deaths appearing globally.
Over the last decade, a potential involvement of autoantibodies against cardiac proteins in the pathogenic processes that either cause or accelerate SCD has been studied.
I highly advise all to read the referenced paper:
Autoantibodies for Cardiac Channels and Sudden Cardiac Death and its Relationship to Autoimmune Disorders
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6367693/
Referenced/Related Papers
Autoantibodies for Cardiac Channels and Sudden Cardiac Death and its Relationship to Autoimmune Disorders
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6367693/
The course of the adaptive response to infection
https://www.ncbi.nlm.nih.gov/books/NBK27125/
Characterization of autoantibodies to endothelial cells in systemic sclerosis (SSc): association with pulmonary fibrosis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1905540/
Autoantibodies Against Human Epithelial Cells and Endothelial Cells After Severe Acute Respiratory Syndrome (SARS)-Associated Coronavirus Infection https://onlinelibrary.wiley.com/doi/epdf/10.1002/jmv.20407
Anti-Endothelial Cell Antibodies are not frequently elevated in hospitalized patients with COVID-19
https://www.mattioli1885journals.com/index.php/actabiomedica/article/view/10799/10548
Mechanisms of Immune Dysregulation in COVID-19 Are Different From SARS and MERS: A Perspective in Context of Kawasaki Disease and MIS-C
https://www.frontiersin.org/articles/10.3389/fped.2022.790273/full
SARS-CoV-2 Spike Protein Suppresses ACE2 and Type I Interferon Expression in Primary Cells From Macaque Lung Bronchoalveolar Lavage
https://www.frontiersin.org/articles/10.3389/fimmu.2021.658428/full
Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs
https://www.sciencedirect.com/science/article/pii/S027869152200206X
Holy smokes. Thanks for all of your hard work putting this together. If what you referenced has been out since 2005, then way more higher ups must be aware of this as a possible outcome. 🤯
Fantastic work Walter!!
Thanks for including all the reference. Scary. Devastatingly scary.
Will be sharing.