


AND THEN THERE WERE NONE: THE SPIKE PROTEIN’S INEXORABLE DESTRUCTION OF THE MICROVASCULATURE AND THE PATHOPHYSIOLOGY OF COVID, LONG COVID AND SADS
If the initial Endothelial assault is not fatal, then recurrent Wound-Heal cycles will be

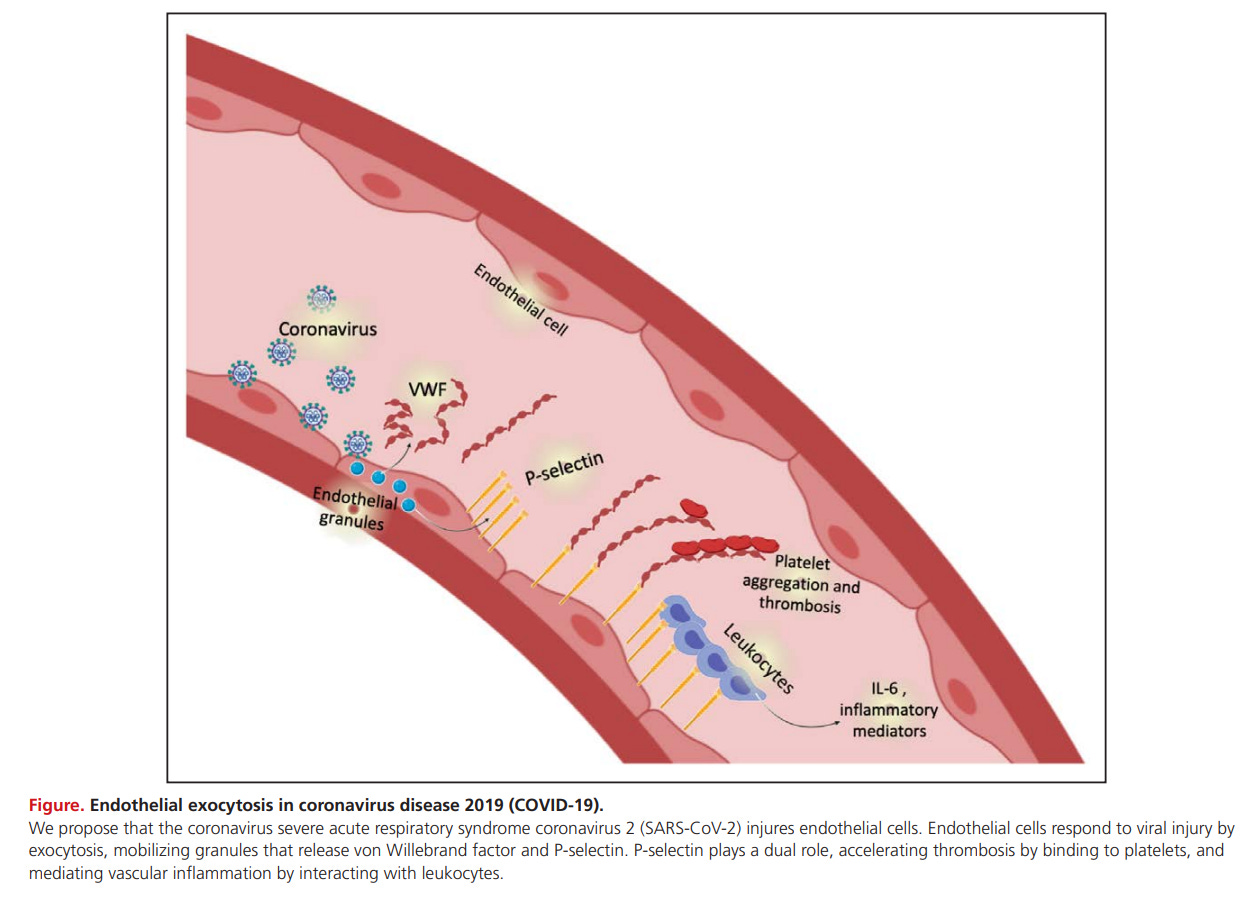
It is well understood that the primary mechanism of death in COVID-19 disease is microvascular in nature.
Severe COVID-19 Is a Microvascular Disease
https://www.ahajournals.org/doi/pdf/10.1161/CIRCULATIONAHA.120.050354
It is also well understood that the Spike Protein damages the Endothelium, and the Endothelial Mitochondria.
Although the use of a noninfectious pseudovirus is a limitation to this study, our data reveals that S protein alone can damage endothelium, manifested by impaired mitochondrial function and eNOS activity but increased glycolysis. It appears that S protein in ECs increases redox stress which may lead to AMPK deactivation, MDM2 upregulation, and ultimately ACE2 destabilization.
SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2
https://www.ahajournals.org/doi/full/10.1161/CIRCRESAHA.121.318902
However, what I believe is not yet well understood is that if the victim survives an infection of SARS-CoV-2, or an exposure to the Spike Protein, irreversible damage has still been done to the Microvasculature of the body. Interestingly, the mechanism of this damage is PRECISELY THE SAME as the mechanism of endothelial damage in DIABETES: THE PATHOGENIC IMBALANCE OF ENDOTHELIAL DAMAGE AND REPAIR.
In health, cumulative damage to endothelial cells incurred by exposure to risk factors is mitigated by endogenous reparative processes. Disruption of the balance between endothelial damage and repair may mediate atherosclerotic progression. Bone marrow-derived ‘endothelial progenitor cells’ (EPC) have been identified as significant contributors to endogenous vascular repair. Insulin resistance is associated with a spectrum of biochemical abnormalities which have the potential to reduce the availability of EPCs and diminish their capacity for vascular repair.
The impact of insulin resistance on endothelial function, progenitor cells and repair
https://journals.sagepub.com/doi/pdf/10.3132/dvdr.2007.027
EXCEPT! With regards to COVID-19 and the Spike Protein, it is not INSULIN that is affecting the availability of Endothelial Progenitor Cells (EPCs). It is the SPIKE PROTEIN!
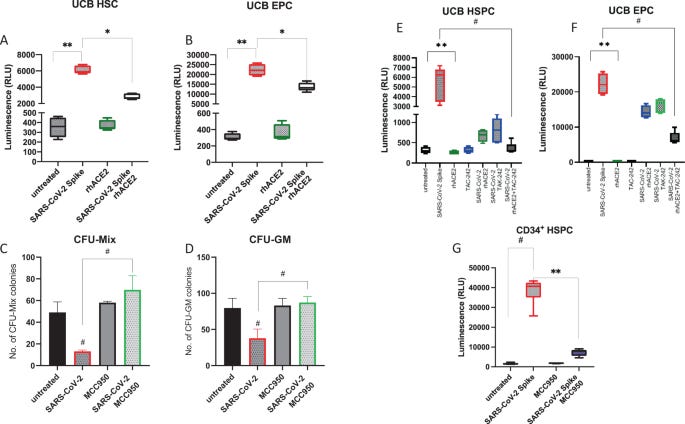
Mounting evidence accumulates that hematopoietic stem/progenitor cells (HSPCs) and endothelial progenitor cells (EPCs) are damaged during severe SARS-Cov-2/COVID-19 infection. It has been reported that patient infected with COVID-19 are frequently presented with anemia, lymphopenia, and thrombocytopenia. This negative effect of the virus on human hematopoiesis and endothelium has been reported in infected patients and demonstrated in vitro after exposure of cells to SARS-Cov-2/COVID-19 spike protein (SP).
An evidence that SARS-Cov-2/COVID-19 spike protein (SP) damages hematopoietic stem/progenitor cells in the mechanism of pyroptosis in Nlrp3 inflammasome-dependent manner
https://www.nature.com/articles/s41375-021-01332-z
And here, I believe, is the major problem:
Both endothelial cells (ECs) and vascular smooth muscle cells (SMCs) are needed for the regeneration of peripheral arteries in ischemic tissues.
Coadministration of endothelial and smooth muscle cells derived from human induced pluripotent stem cells as a therapy for critical limb ischemia
https://stemcellsjournals.onlinelibrary.wiley.com/doi/full/10.1002/sctm.20-0132
Yet, there are not enough Endothelial Progenitor Cells available to repair the damage. This is like trying to make a Hollandaise sauce with just egg yolks – and no butter. I believe this explains the lumen narrowing which I believe is occurring because of this impaired repair process. Yielding the same results as the impaired microvascular repair response seen in Diabetes.
Diabetic patients have increased VSMC proliferation and switch to a more synthetic phenotype consistent with vascular dysfunction, which can produce medial layer thickening and narrowed lumen of the artery which results in ischemia.
Diabetic vasculopathy: macro and microvascular injury
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7351096/
So, as one can deduce, if a damaged endothelium is REDAMAGED and REDAMAGED over and over again, and CANNOT BE HEALED PROPERLY EACH TIME, eventually the microvasculature will vanish - and become scar tissue and/or smooth muscle.
Unfortunately, I do not believe this is the only fatal mechanism of the Spike Protein. From what I have observed, the Spike Protein has the “unique” (to say the least) to INDUCE DAMAGE AND SIMULTANEOUSLY IMPAIR THE RESPONSE NEEDED TO REPAIR THE DAMAGE IT CAUSES.
This has been a full explanation of how the Spike Protein is either immediately, or progressively, inducing fatal microvascular damage. I am working on detailing how this affects all systems of the body, and how this explains the observed symptoms of Long COVID and the dramatic increase in SADS.











So whether vaccinated or not, we are screwed? Since most all of us have had covid , and will continue to get it as it is mutating regularly?
I think perhaps 'Long Covid' should be reserved as a diagnosis only appropriate for a small and unfortunate number of strictly unvaccinated people who caught Covid and haven't managed to fight off the effects, perhaps because their immune systems aren't fully operational for whatever reason (not Covid related). However for the "vaccinated", I think what is being referred to as "Long Covid" should perhaps be renamed "Long Vaccine"