

WORKING: THE AUTOIMMUNITY (AND PRION DISEASE) BEING OBSERVED POST COVID-19 AND SPIKE PROTEIN EXPOSURE MAY BE DUE TO THE INJURY CAUSED BY THE SPIKE PROTEIN (S1 UNIT IN PARTICULAR)
Traumatic Brain Injury and Inclusion Body Myositis as precedent - is SPED, SPID? (Spike Protein Injury Disease)

I believe I may have solved, or at least found a very significant piece of, the occurrence of autoantibodies in those who have had COVID-19 and/or exposure to the Spike Protein of SARS-CoV-2.
The SITE OF DAMAGE can present autoantigens to B-Cells, inducing autoantibodies.
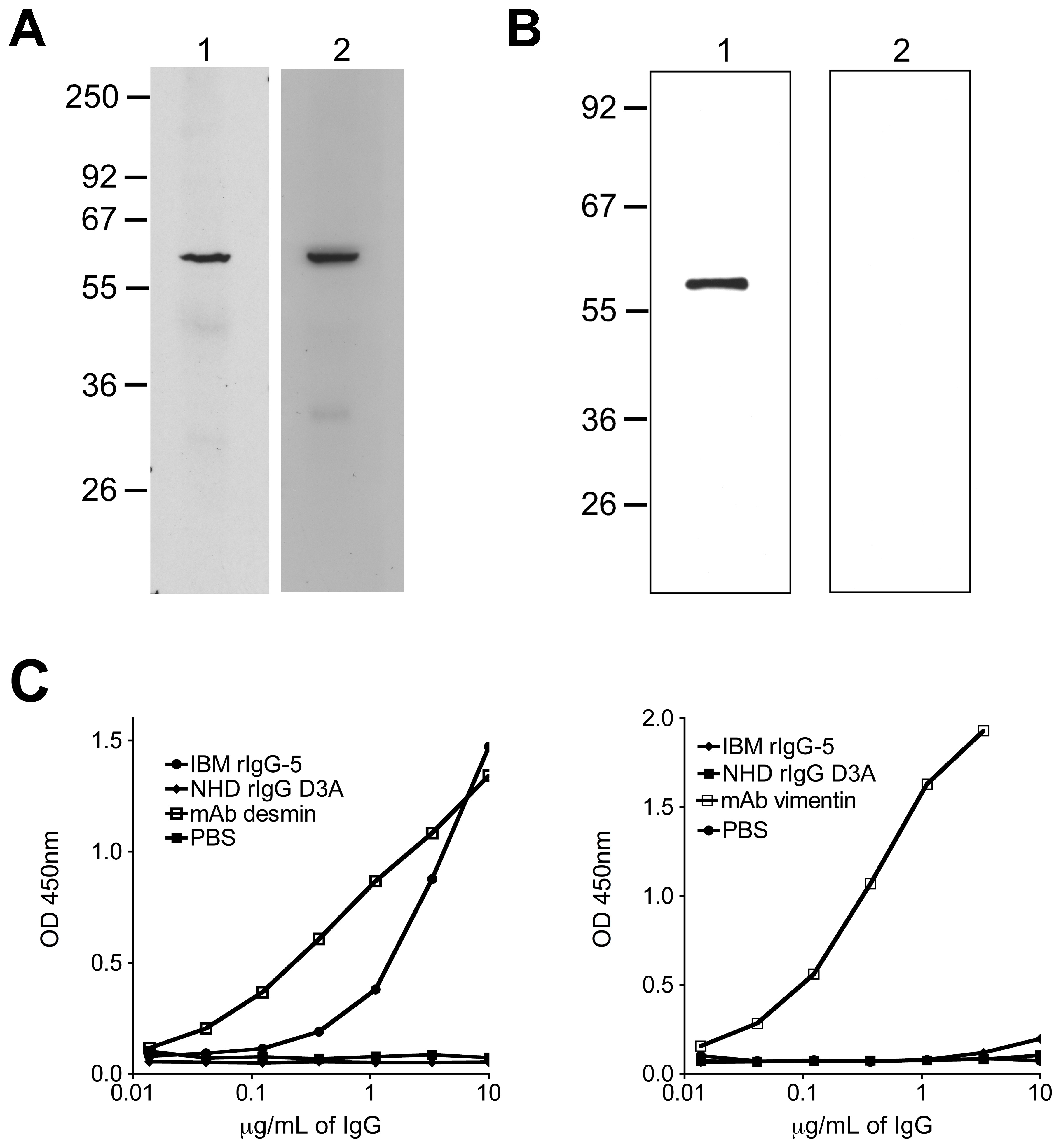
Having determined that IBM serum harbors self-reactive immunoglobulin, we next focused our study at the site of IBM tissue injury. Earlier studies, from our group and others, established that antigen-experienced plasma cells reside in IBM muscle tissue. Thus, we reasoned that autoantigens present in the damaged tissue might be the target of the antibodies produced at this site.
Our observation that several of the rIgG derived from IBM muscle specific plasma cells recognized self-antigens, prompted us to search for their antigenic targets.
Autoantibodies Produced at the Site of Tissue Damage Provide Evidence of Humoral Autoimmunity in Inclusion Body Myositis
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0046709
The same is true in Traumatic Brain Injury.
Of interest, is the occurrence of autoantibodies which are produced following CNS trauma-induced disruption of the blood-brain barrier (BBB) and released into peripheral circulation mounted against self-brain-specific proteins acting as autoantigens.
Autoantibodies in traumatic brain injury and central nervous system trauma
https://pubmed.ncbi.nlm.nih.gov/25220901/
If, by logical extension, we assume the same pathogenesis is occurring at other sites of Spike Protein (in particular, the S1 Unit) damage, this may satisfactorily explain the heterogeneity of autoimmune responses in those exposed to the Spike Protein of SARS-CoV-2.
UPDATE: I believe this also applies to the rapid incrase in observed cases of Prion disease.
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease associated with repetitive traumatic brain injury (TBI). CTE is generally found in athletes participating in contact sports and military personnel exposed to explosive blasts but can also affect civilians. Clinically and pathologically, CTE overlaps with post-traumatic stress disorder (PTSD), a term mostly used in a clinical context. The histopathology of CTE is defined by the deposition of hyperphosphorylated tau protein in neurons and astrocytes preferentially with perivascular distribution and at the depths of the cortical sulci. In addition to hyperphosphorylated tau, other pathologic proteins are deposited in CTE, including amyloid β (Aβ), transactive response (TAR) DNA-binding protein 43 kDa (TDP-43) and α-synuclein. However, the coexistence of prion disease in CTE has not been observed. We report three cases of histopathologically validated CTE with co-existing sporadic prion disease.
Co-occurrence of chronic traumatic encephalopathy and prion disease
https://actaneurocomms.biomedcentral.com/articles/10.1186/s40478-018-0643-9
Of course, feedback is welcome as I work on this aspect of Spike Protein pathology.
As always, thank you for your support.
Myositis describes a few of my vaxxed friends to a tee. As always I believe you are on the right track.
How long has the spike protein really been around? Could they have used it in other vaccines without disclosing? I don’t doubt that your info on the spike is true, but I think there may be other mechanisms working with vaccines in general. My daughter was diagnosed with Hashimoto’s thyroiditis & +ANA after the Guardisil vaccine a few years ago. She did not receive the covid vax. I know she is my n=1, but there’s a lot of Hashi’s in young women now, so she may just be one of many.