

The Spike Protein, MHC 1 and Autoimmune Disease
How the Spike Protein can turn one's organs into "transplants."

Three years ago, in 2021, I wrote that due to the massive peptide sharing the Spike Protein of SARS-CoV-2 has with human proteins (twenty-six peptide sequences), autoimmunty would inevitably develop. Especially with repeated exposures.
SEVERE COVID, MIS-C, MIS-A, MIS-V, LONG COVID AND AUTOIMMUNITY: MOLECULAR MIMICRY OF THE SARS-CoV-2 SPIKE PROTEIN AS “GRAFT,” ITS ACTIONS IN COVID-19 AND GRAFT VS HOST DISEASE: DISEASES OF TARGET TISSUE DESTRUCTION
https://wmcresearch.org/covid-19-and-graft-vs-host-disease/
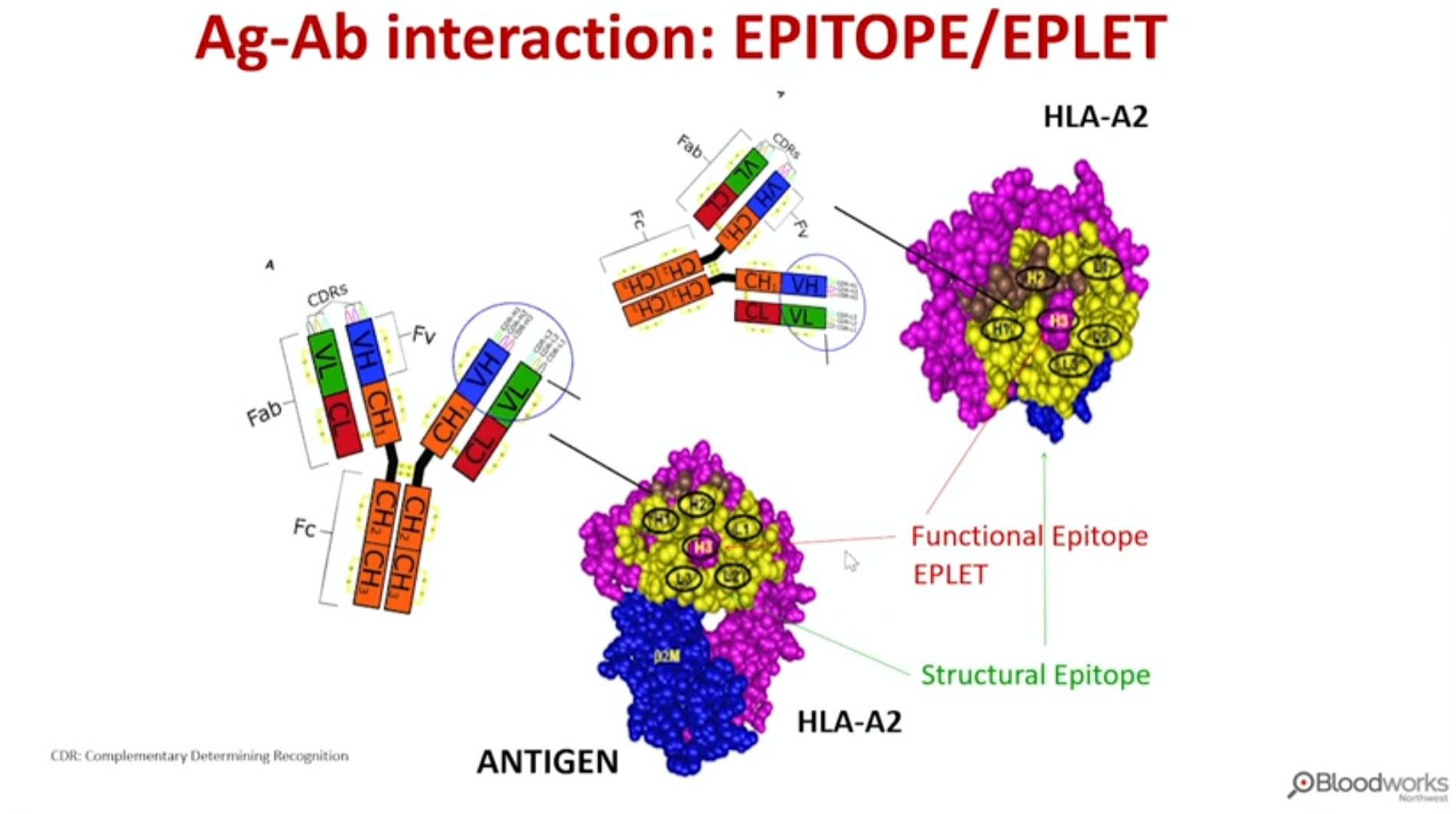
The mechanism for this I can now more fully describe - interestingly from an article published the same year - which I have recently discovered. Just as in organ transplant rejection, the immune system attacks HLAs. The peptides displayed on HLAs from our cells "grinding up" Spike Proteins causes our immune system to view the HLA-peptide complex as foreign. I will now share those discrete sequences in the Spike Protein.
The RRARSVAS peptide is found in a neutralizing B-cell epitope of SARS-CoV-2 surface glycoprotein (99). Moreover, RRARSVAS is located near to motif responsible for super-antigenicity property of the spike protein. This epitope is located close to the S1/S2 cleavage site of the spike protein and resembles the super-antigen motif from Staphylococcal enterotoxin B (SEB). This sequence could be the possible explanation for cytokine storm in severe COVID-19 patients and multisystem-inflammatory syndrome (MIS-C) observed in children (100, 101). This sequence is also found in T-cell epitopes of SARS-CoV-2 spike protein. These T-cell epitopes are known to bind to various HLAs, including those associated with ADs (HLA-B*08:01 and HLA-B*07:02) (102–104). Moreover, the RARSVA sequence is found in an 11-meric epitope derived from a human antigen. This 11-meric epitope is known to bind to HLA-A*66:01 allele. The HLA-B*08:01 is associated with myasthenia gravis (105), and the HLA-B*07:02 is associated with neurological ADs (85). Reports are available about myasthenia gravis associated with SARS-CoV-2 infection (68, 106–108). Surface glycoprotein is the leading antigen of interest for vaccine development against SARS-CoV-2 (109). DEDDSEPV peptide is conserved in B-cell epitopes of SARS-CoV-2 and SARS-CoV-1 surface glycoproteins (110–113). Moreover, this peptide has recently been found in a 10-meric T-cell epitope of SARS-CoV-2 spike protein. This epitope is reported to bind to HLA-B*40:01 allele (102). The DDSEPV sequence has also been found in an epitope derived from a human antigen. This epitope is known to bind to various HLAs, including those associated with ADs (e.g., HLA-B*27:05 and HLA-C*08:01) (114, 115). Hence, vaccine candidates harboring either of these two peptides (DEDDSEPV and RRARSVAS) could be harmful considering the ADs development. The RRARSVAS peptide could be assigned as the most harmful peptide, since it is found in a neutralizing B-cell epitope of SARS-CoV-2. Therefore, this epitope could be of interest in vaccine design and formulation.
SARS-CoV-2 Proteome Harbors Peptides Which Are Able to Trigger Autoimmunity Responses: Implications for Infection, Vaccination, and Population Coverage
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8383889/
Why this has not been shouted from the rooftops, I will never understand. I will continue to work on further understanding of this mechanism, and ways to inhibit it. There is much to unpack here, including the super-antigen motif mimicry of the RRARSVAS sequence.
Thank you, as always, for your readership, dialog and support.
Or is this another toxin we might find residual in the jabs?
Staphylococcal enterotoxin B (SEB) is the prototype of a non-egc-associated potent SAg. It is categorized as a category B select agent because it is the most potent staphylococcal enterotoxin, and much lower quantities are sufficient to produce a toxic effect than with synthetic chemicals. Furthermore, SEB is extremely stable and easily produced in large quantities. At low concentrations, SEB can cause multi-organ system failure and death. During the 1960s, when the United States had an offensive biological warfare program, SEB was studied as a biological weapon and stockpiled with various other bioweapons prior to its destruction in 1972 (4). Based on those investigations, the effective dose of SEB that would incapacitate 50% of the exposed population was estimated to be 0.0004 μg/kg of body weight, whereas the 50% lethal dose was estimated to be 0.02 μg/kg of body weight for humans exposed by the inhalation route. A convention on the “Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction” was signed by the United Kingdom, U.S., and U.S.S.R. governments in 1972. The U.S. government opted to reestablish research programs for vaccine and therapeutic development against biological weapons after suspicion arose that the U.S.S.R. was continuing the stockpiling and testing of biological weapons. Major NIH grant funding reinvigorated research on biological warfare agents after 11 September 2001 and especially after the anthrax attacks occurred in the U.S. mail system. Despite extensive efforts, however, there is no therapy or vaccine approved for human use against SEB to date.
Yep. This is another fine mess.
Yet it was - April 2020 - #PathogenicPriming - see 225 citations of the first study to propose it - https://scholar.google.com/scholar?cites=13864713792690032167&as_sdt=80000005&sciodt=0,23&hl=en I like the analogy that the spike protein can turn your organs (and tissues) into transplants, Walter.