

The Spike Protein and IL-6: Persistent Low-Level Inflammation as Cause of Sudden Cardiac Death (SCD)
Is the Spike Protein inducing “Fast” and “Slow” SCDs? From fulminant myocarditis to sustained IL-6 elevation.

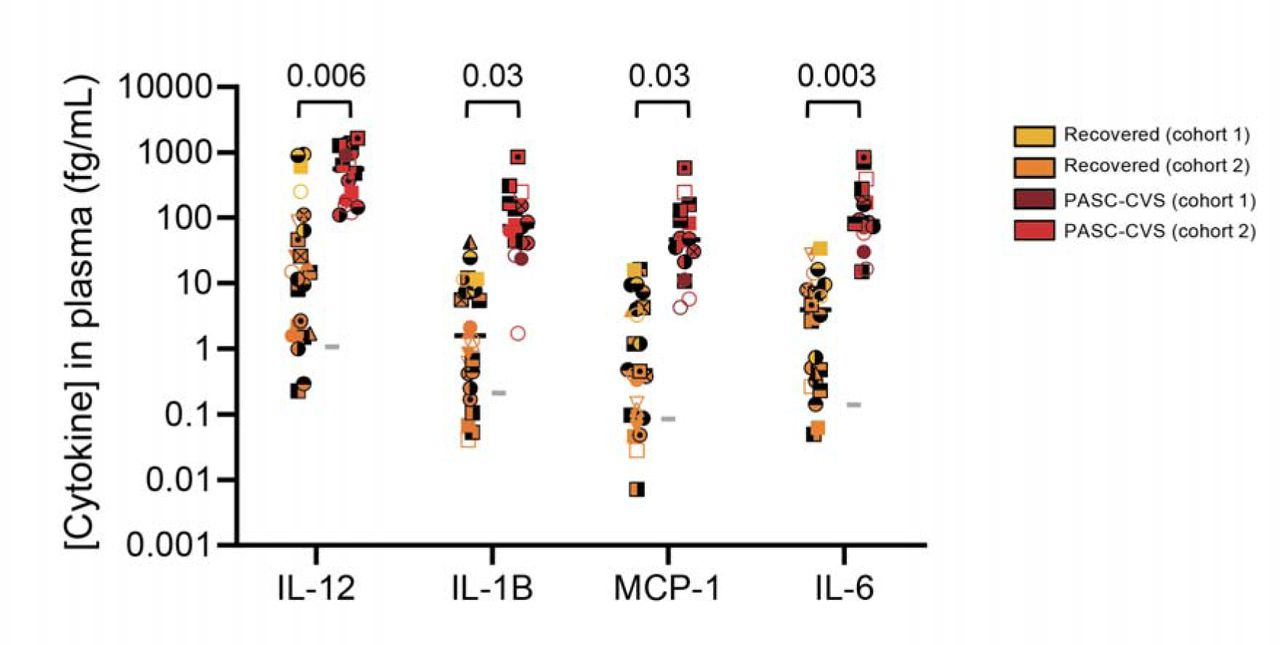
Nanotechnology can detect elevated cytokine levels in the plasma of individuals with PASC-CVS.
Cytokine levels detected in the plasma of participants by immunostormchip. Median is shown in all graphs by a black bar. Statistical significance was determined with an ANCOVA adjusted for age, sex and/or site as covariates. Covariates were included in the analysis if statistically significant difference in the covariate was recorded between groups. Each donor is indicated by a unique symbol that is used consistently throughout all figures. Grey horizontal lines indicate the mean value derived from n = 9 Healthy donors.
One of the most disturbing and puzzling phenomena the world now faces since the Spike Protein was “introduced,” is that many young people, especially athletes, are suddenly dying from cardiac events. Many researchers, me included, have proposed hypotheses to explain how this may be occurring. All those theories still hold as potential causes. However, I would like to add one more, given recent findings.
A very interesting paper was published earlier this year, which I referenced in one of my posts earlier this month.
In this cross-sectional study, blood samples were obtained from three different sites in Australia from individuals with i) a resolved SARS-CoV-2 infection (and no persistent symptoms i.e. ‘Recovered’), ii) individuals with prolonged PASC-CVS and iii) SARS-CoV-2 negative individuals. Individuals with PASC-CVS, relative to Recovered individuals, had a blood transcriptomic signature associated with inflammation. This was accompanied by elevated levels of pro-inflammatory cytokines (IL-12, IL-1β, MCP-1 and IL-6) at approximately 18 months post-infection. These cytokines were present in trace amounts, such that they could only be detected with the use of novel nanotechnology. Importantly, these trace-level cytokines had a direct effect on the functionality of pluripotent stem cell derived cardiomyocytes in vitro. This effect was not observed in the presence of dexamethasone. Plasma proteomics demonstrated further differences between PASC-CVS and Recovered patients at approximately 18 months post-infection including enrichment of complement and coagulation associated proteins in those with prolonged cardiovascular symptoms. Together, these data provide a new insight into the role of chronic inflammation in PASC-CVS and present nanotechnology as a possible novel diagnostic approach for the condition.
Cardiovascular symptoms of PASC are associated with trace-level cytokines that affect the function of human pluripotent stem cell derived cardiomyocytes
https://www.biorxiv.org/content/10.1101/2024.04.11.587623v1.full
What made this of particular interest to me is that those suffering from PASC also have Spike circulating in their blood.
This study, in agreement with other published investigations, demonstrates that both natural and vaccine spike protein may still be present in long-COVID patients, thus supporting the existence of a possible mechanism that causes the persistence of spike protein in the human body for much longer than predicted by early studies. According to these results, all patients with long-COVID syndrome should be analyzed for the presence of vaccinal and viral spike protein.
Presence of viral spike protein and vaccinal spike protein in the blood serum of patients with long-COVID syndrome
https://www.europeanreview.org/article/34685
Now, the above study was retracted because the editor “mistrusts the results” though the authors – correctly – disagree.
The outcome of the investigation revealed that the manuscript presented major flaws in the following: - Unclear methodology and patient recruitment - Discrepancies among data reported in the text and tables - Unreliable results - Undeclared conflict of interest Consequently, the Editor in Chief mistrusts the results presented and has decided to withdraw the article. The authors disagree with this retraction. The Publisher apologizes for any inconvenience this may cause.
I read the study and find it to be completely sound. Please decide for yourself.
When we add to the above that the Spike is solely responsible for the elevated levels of IL-6, a very clear picture begins to emerge.
We observed that spike (S) protein potently induced inflammatory cytokines and chemokines, including IL-6, IL-1β, TNFα, CXCL1, CXCL2, and CCL2, but not IFNs in human and mouse macrophages. No such inflammatory response was observed in response to membrane (M), envelope (E), and nucleocapsid (N) proteins.
SARS-CoV-2 spike protein induces inflammation via TLR2-dependent activation of the NF-κB pathway
https://elifesciences.org/articles/68563#content
For reasons yet unknown (genetic?) there are those that have an inflammatory response to the Spike Protein which results in fulminant myocarditis, and there appears to be those who have a very low-level, sustained inflammatory response to the Spike Protein which can explain the sudden cardiac deaths, especially in athletes.
Myocardial/pericardial inflammation is relatively common in athletes, and can portend potentially ominous complications, including sudden cardiac death. A thorough patient evaluation, including CMR, and (EVM-guided) EMB is key for successful management and can provide essential data for the safe assessment of sports eligibility and for the estimation of prognosis. The care athletes with myocarditis or chronic ICM (inflammatory cardiomyopathy) is best accomplished in centers with considerable expertise [60], given the multiple challenges encountered in the diagnosis, treatment, and follow-up of these patients.
Myocardial Inflammation, Sports Practice, and Sudden Cardiac Death: 2021 Update
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8002711/
Furthermore, this slow-burn “accelerated aging (inflammaging)” can also explain SCD in non-athletes. IL-6 is the culprit.
RESULTS
In univariate analyses, both IL-6 (hazard ratio [HR] 1.79 for 1þ log IL-6, 95% confidence interval [CI] 1.50–2.13; 5th vs 1st quintile HR 3.36, 95% CI 2.24–5.05) and CRP (HR 1.31 for 1þ log CRP, 95% CI 1.18–1.45; 5th vs 1st quintile HR 2.00, 95% CI 1.40– 2.87) were associated with SCD risk. In covariate-adjusted analyses, accounting for baseline risk factors, incident myocardial infarction, and heart failure, the association with SCD risk persisted for IL-6 (HR 1.26 for 1þ log IL-6, 95% CI 1.02–1.56; 5th vs 1st quintile HR 1.63, 95% CI 1.03–2.56) but was significantly attenuated for CRP (HR 1.13 for 1þ log CRP, 95% CI 1.00–1.28; 5th vs 1st quintile HR 1.34, 95% CI 0.88–2.05). Similar findings were observed in participants without prevalent cardiac disease.CONCLUSION
Greater burden of inflammation, assessed by IL-6 levels, is associated with SCD risk beyond traditional risk factors, incident myocardial infarction, and heart failure.
Inflammation and sudden cardiac death in a community-based population of older adults: The Cardiovascular Health Study
https://www.heartrhythmjournal.com/article/S1547-5271(13)00729-7/pdf
We certainly need population-wide screening to determine presence of Spike. Of course, if you don’t look for something, you won’t find it. The human body is a fine-tuned machine. A persistent, inexorable nudging towards a cliff will certainly push one over it.
Thank you, as always, for your readership, dialog and support.
When a paper is withdrawn by an editor, to me, that is a confirmation that the paper is uncovering the truth. These days the people in power don’t want the rest of us to know what the truth is.
Thank you Walter. May God bless you and guide you. Peace.