

The Depletion of ACE2 and Sudden Cardiac Death: Lessons from SARS
We may need to radically rethink the Spike Protein: Cancer spreads taking over metabolism – the Spike spreads depleting ACE2.

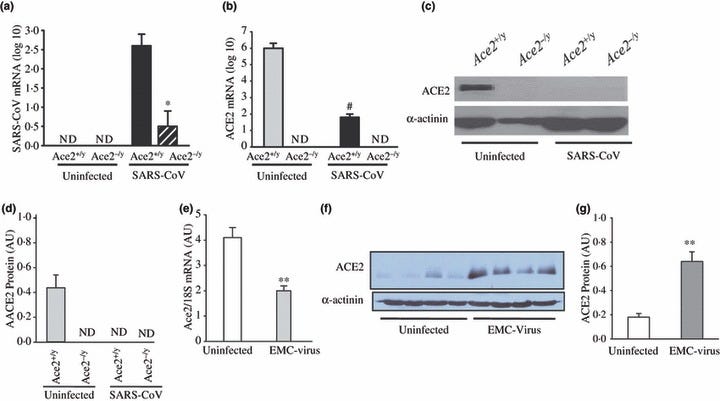
Pulmonary SARS‐CoV infection leads to myocardial SARS‐CoV infection and down‐regulation of myocardial ACE2 expression. (a–d) Human SARS‐CoV mRNA in the hearts of infected mice showing a clear dependence on ACE2 for myocardial SARS‐CoV infection (a) with down‐regulation of myocardial Ace2 mRNA expression based on real‐time PCR (b) and myocardial ACE2 protein levels shown by Western blot analysis (c) and quantification (d) in response to pulmonary SARS‐CoV infection. *P < 0·01 compared with infected Ace2+/y group; #P < 0·01 compared with uninfected group, n = 5, ND, not detectable. (e–g) Discordant changes in myocardial Ace2 mRNA and myocardial ACE2 protein levels in encephalomyocarditis (EMC) virus‐induced myocarditis with real‐time PCR showing reduced myocardial Ace2 mRNA (e) with increased myocardial ACE2 protein levels based on Western blot analysis (f) and quantification (g). **P < 0·01 compared with placebo group, n = 5.
A paper from 2009 made a very interesting, and incredibly relevant to today’s situation, observation about the interaction of SARS with ACE2. This is without question due to the presence of the Spike Protein which utilizes ACE2 as its docking receptor. The discussion begins with a very important statement, one which vaccine developers should have had front and center from the beginning of their development process.
Patients who were infected with the SARS virus suffered from cardiac disease ranging from systolic and diastolic dysfunction, arrhythmias and sudden death.
Moreover, the ACE2 protein was COMPLETELY ELIMINATED in those whose hearts were infected with SARS. This was an astounding 35% of patients. That figure should be taken as extremely conservative in the context of SARS-CoV-2 as its Spike Protein is FAR MORE effective at binding ACE2.
The complete loss of ACE2 protein in hearts infected with SARS‐CoV could be secondary to the activation of ADAM‐17/TACE by the SARS spike protein, which is known to cleave and release ACE2 and/or due to SARS‐CoV binding to ACE2 in the endothelial cells leading to endocytosis of the ligand/receptor complex and subsequent intracellular degradation of ACE2.
SARS‐coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7163766/
What does this mean? It offers a solid and indisputable explanation for the plethora of sudden cardiac deaths we are now observing. Please bear in mind that we need to look at multiple mechanisms for sudden cardiac death. Clearly, the direct induction of myocarditis is a major factor as well as sudden death due to neurological issues. However, I believe the evidence shows that ACE2 depletion may be the eminence grise behind the vast majority of the observed sudden cardiac deaths.
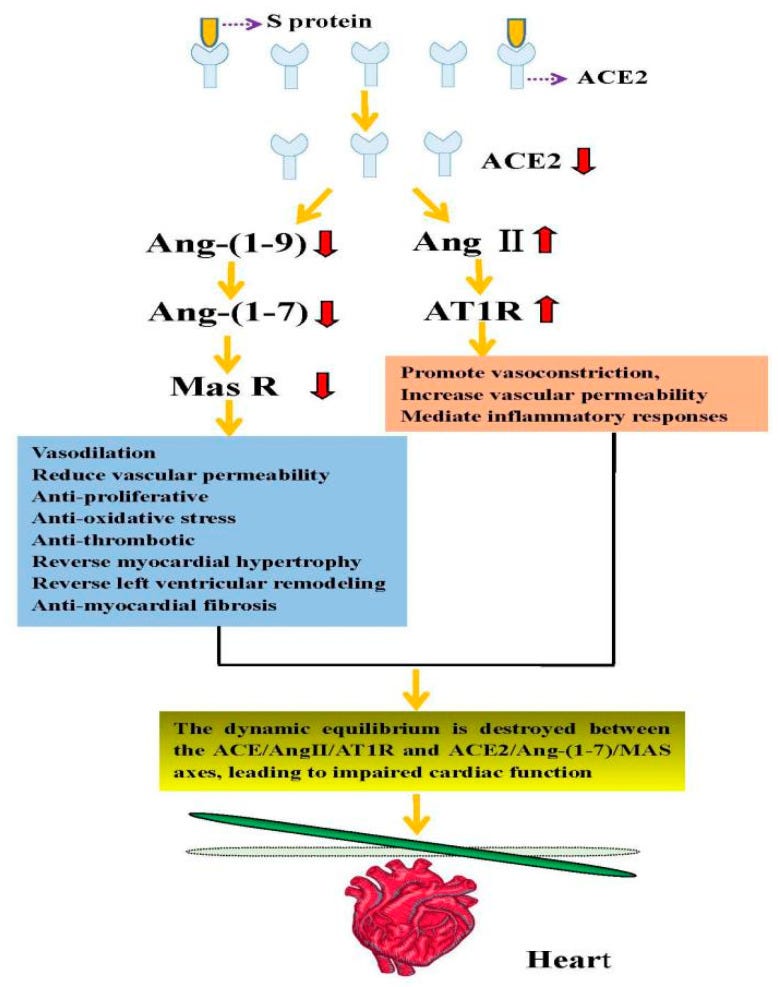
The direct mechanism of cardiac injury caused by SARS-CoV-2 using ACE2 as the target. Angiotensinogen is converted to Ang I by renin. Angiotensin-converting enzyme (ACE) can convert Ang I into Ang II, which in turn can activate the angiotensin II type 1 receptor (AT1R). ACE2 can cleave Ang I to produce the Ang-(1-9) peptide, which can then be converted into the vasodilator peptide Ang-(1-7) through ACE or other peptidases. Conversely, ACE2 can hydrolyze Ang II into Ang-(1-7), which acts on Mas receptors. When the SARS-CoV-2 S protein binds to ACE2 receptors, the dynamic equilibrium is destroyed between the ACE/Ang II/AT1R and ACE2/Ang-(1-7)/MAS axes, leading to impaired cardiac function.
Previous studies have shown that the function of ACE2 is lost when SARS-CoV-2 binds to ACE2, which counteracts the cardioprotective effect of ACE2. Besides, this will create a vicious circle, aggravating heart damage. Further investigation revealed that the patient’s serum Ang II levels were significantly elevated. This finding may be because once the human body is infected with SARS-CoV-2, ACE2 will be depleted, which will affect the dynamic equilibrium between ACE2/Ang-(1-7)/MAS and ACE/Ang II/AT1R axes, eventually leading to impaired cardiac function.
Research Progress on the Cardiac Injury from ACE2 Targeting in SARS-CoV-2 Infection
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7911115/
One may then surmise that increasing expression of ACE2 would be beneficial. However, we encounter the same problems by overexpressing the gene.
On the other hand, transgenic mice with increased cardiac ACE2 expression had a high incidence of sudden death due to progressive conduction and rhythm disturbances with sustained ventricular tachycardia and terminal ventricular fibrillation. Thus the exact role of ACE2 in cardiovascular disease, and in particular heart disease, remains incompletely understood.
Renin–angiotensin system blockade in the COVID-19 pandemic
https://academic.oup.com/ckj/article/14/Supplement_1/i48/6126370
We are faced with quite a dilemma. We are walking a lethal tightrope. As virtually everything regarding health, imbalance and dysregulation can lead to disastrous consequences.
Perhaps we need to rethink the Spike Protein. Whereas HIV patients must monitor levels of HIV, humanity may be forced to monitor levels of Spike Protein. After all, cancer kills because the proliferation of cancer cells eventually take over the body’s metabolism. HIV kills because it eventually depletes CD4+ T Cells and the Spike Protein kills (among many reasons) by depleting ACE2.
I am concerned by those who state that COVID is not a threat. Perhaps the Acute version of COVID is no longer an immediate threat, but those Spike Proteins are circulating (and being forced upon us) incrementally depleting our bodies of this absolutely critical protein. For now, finding ways to reduce Spike load may be the best approach we have towards mitigation.
I’m type O blood and have chewed nicotine gum the past 2 years…I also take Dr. VanDeWater’s spike recovery because I’m around folks every day that have taken the gene therapy shots. When I was pregnant 2-1/2 years ago with my 3rd son I started researching to prove to my Obgyn why I wouldn’t take their shots. 2 different doctors lectured me on why it was a necessity for the health of my baby and me, but I stood strong and collected research to show them and prove why I would not be conforming. They thought I was cra-cra, but I didn’t care.
The information below is from NIH’s website, and they knew exactly what they were doing. It’s been planned for decades. One example is close to my heart and I have long suspected that there were other motives as to why I have so many half siblings. In the 1970s & 80s, UNMC had a sperm donor program through the Munroe-Meyer Institute that med students donated to. I met with Dr Warren Sanger and Dr Bruce Buehler, who headed this program up, when I was on the quest to find out my genetics and find my donor. The max offspring for each donor was 8 (unless you were type O blood type). The donor that I came from is type O and they used his sperm dozens of times. I’ve found many of my half siblings and my bio dad. He tried to find out how many times they used it and UNMC isn’t disclosing this information. My bio dad thinks there could be many more, and guess what we’re all type O.
From NIH’s website:
On the contrary, the A allele of the ABO blood group has been associated with an increased risk of developing cardiovascular diseases as reported by several studies.10 The A antigen might protect P-selectin and intercellular cell adhesion molecule 1 (ICAM1) from enzymatic cleavage by promoting stronger and longer binding of leukocytes to them on the vascular wall; more adhesion molecules attached to the endothelial cells would on one hand increase adhesion and inflammation but on the other hand decrease circulation.11 These collectively predispose type A carriers to a higher likelihood of developing cardiovascular diseases and aggregate disease situations once these individuals were exposed to redox stresses such as in the case of virus infection.
Therefore, individuals having an O blood group type are less likely to develop cardiovascular diseases and severe COVID-19 and, on the contrary, patients carrying an A blood group type, especially those already having been diagnosed with cardiovascular diseases in particular hypertension, are more likely to develop severe COVID-19 once infected (Figure 1). These individuals need to be quarantined and protected from SARS-CoV-2 infection or under special medical care to be prevented from deterioration and severe progression.
These Bioweapon designers play to win.