

The Cases Of Vaccine Lung Transplant Rejection As Cases Of Advanced Instances Of SPED: Why COVID/Long COVID/SPED Mimics Graft vs Host Disease
Attributed To Antibody Mediated Rejection, Actually C4D Complement Deposition Induced By The Spike Protein

In April of this year (2022), a paper was published which demonstrated that patients who had received a lung transplant were experiencing Lung Transplant Rejection (LTR) due to what appeared to be Antibody Mediated Rejection (AMR).
Limited antibody response to messenger RNA (mRNA) vaccines has been reported in LTR, with the majority mounting a response after the 2nd dose. In this series, 3 patients developed new and significant respiratory compromise after their 2nd vaccine dose consistent with antibody mediated rejection (AMR).
COVID-19 Vaccine Triggered Rejection in Lung Transplant Recipients: A Case Series
https://www.sciencedirect.com/science/article/pii/S1053249822013705
The operative words above are “consistent with.” However, what actually is Antibody Mediated Rejection? It is an endothelial disorder!
Antibody-mediated rejection (AMR) of solid organ transplants is characterized by the activation and injury of the allograft endothelium.
The Role of the Endothelium during Antibody-Mediated Rejection: From Victim to Accomplice
https://www.frontiersin.org/articles/10.3389/fimmu.2018.00106/full
I believe the most critical factor to understand here, is that Organ Transplantation itself is very disruptive to the endothelium. The endothelium is already damaged, as it is in all risk factors for Severe COVID.
At long last I see the bridge to the similarity of Graft vs Host disease and COVID/Long COVID/SPED. Those who have been following my work will recall the observation I made long ago. Please search my substack and research website for the relevant posts.
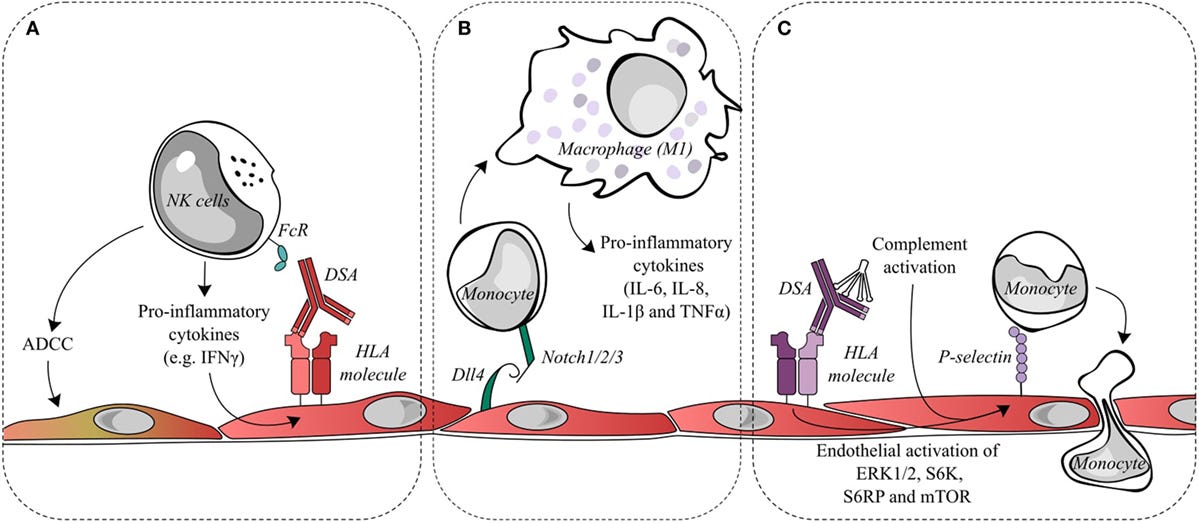
Organ transplantation, however, subjects the endothelium to an environment of inflammation, alloreactive lymphocytes, donor-specific antibodies, and potentially complement activation. As a result, endothelial cells become activated and have modified interactions with the cellular effectors of allograft damage: lymphocytes, natural killer, and myeloid cells. Activated endothelial cells participate in leukocyte adhesion and recruitment, lymphocyte activation and differentiation, as well as the secretion of cytokines and chemokines. Ultimately, highly activated endothelial cells promote pro-inflammatory alloresponses and become accomplices to AMR.
The Role of the Endothelium during Antibody-Mediated Rejection: From Victim to Accomplice
https://www.frontiersin.org/articles/10.3389/fimmu.2018.00106/full
But, what causes this in AMR, if it is not antibodies? It is complement deposition. This is why the authors observed their findings were CONSISTENT WITH AMR.
In the case of renal transplantation, AMR is identified by the presence of circulating donor-specific antibodies (DSAs), morphologic evidence for tissue injury such as transplant glomerulopathy (characterized by reduplication of glomerular basement membranes), and evidence for antibody interaction with the vascular endothelium such as C4d deposition and/or microvascular inflammation.
The Role of the Endothelium during Antibody-Mediated Rejection: From Victim to Accomplice
https://www.frontiersin.org/articles/10.3389/fimmu.2018.00106/full
So, as you can see, it is not necessary to have antibody interaction to induce AMR. You need C4d deposition and/or microvascular inflammation. The Spike Protein provides both.
More direct evidence for the contribution of C to tissue damage was obtained from postmortem analysis of 2 lung and 3 skin biopsy specimens of COVID-19 patients that revealed deposits of C activation products C4d, C3d and C5b-9 in the lung inter-alveolar septal microvessels and in the skin vasculature.
Multi-organ complement deposition in COVID-19 patients
https://www.medrxiv.org/content/10.1101/2021.01.07.21249116v1.full-text
Clearly, it must be the Spike Protein inducing this deposition as it is the only viral protein expressed via mRNA vaccination.
So, what is the most important question to ask? What is the most important study we need to perform?
We must learn what happens to the endothelium when exposed to Spike Protein in healthy subjects without any pre-existing conditions or comorbidities.
I am eternally grateful for your support. I will continue to work. Blessings in this holiday season.
Thank you very much Walter. May God bless you and continue to guide you in your very important work. Thank you for caring and for always telling the truth.
Yes,Walter. Our hospital system stopped any vax or boosters for transplants of any kind, but particularly heart/lung. Very poor outcomes in those getting "freshly" "vaxxed" or boosters just meet that requirement. These were pts who would never have done vax, declined or had such contraindications - just no. No way.
Very poor outcomes. Just say, death. Rejection on a scale that they just quietly dropped the requirement. Can't do anything about previous injections, but nothing just prior now. I do know these pts are being tracked for research - successful and those who had earlier jabs ... unfortunately, no one has yet truly connected transplant need in many to taking jabs. At least not publicly.