Stored Toxin vs. Continual Expression: The Spike Protein, Agent Orange and a Diagnosis after Forty Years
When we observe the parallel effects of bioaccumulating toxins like Agent Orange and the continual expression of proteins like the Spike Protein, long-term pathology should be on our radar.

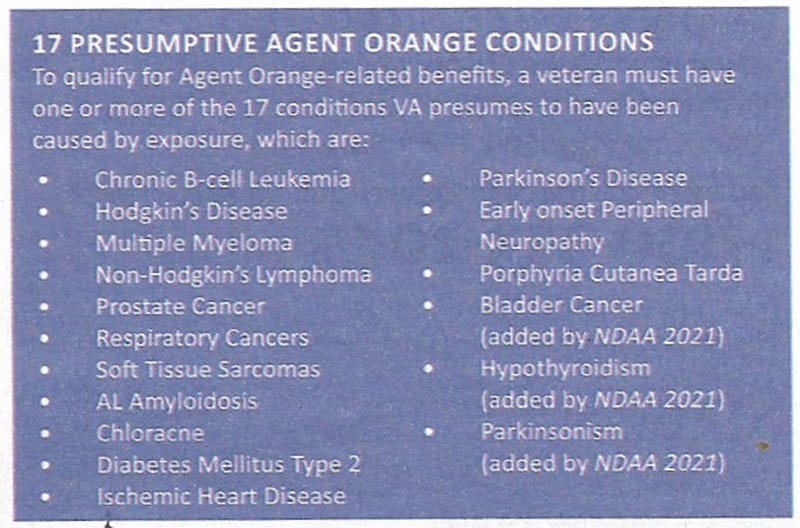
Presumptive Agent Orange conditions.
There is a story I would like to share about an individual who was exposed to Agent Orange half a century ago. This individual developed amyloidosis forty some years after being exposed to Agent Orange. Please read the story carefully – and please think of the Spike Protein as you read it.
Amyloidosis and Agent Orange
Szymanski, 74, of Centennial, is a retired real estate developer and avid cyclist whose run-in with amyloidosis can be traced back to his service in Vietnam. He spent 1969-1970 leading a platoon there, having been drafted after attending the University of Denver. The U.S. Veterans Administration provides health care and disability compensation for amyloidosis patients exposed to Agent Orange and other herbicides during their military service in Vietnam.
Szymanski was a serious cyclist, one fit enough to ride the 110-mile Triple Bypass into his 50s. He had never been treated in a hospital until 2013, when stabbing abdominal and lower-back pain of mysterious origins emerged. A series of tests – a lymph-node biopsy, a gallbladder biopsy, an endoscopy, a colonoscopy, and others – led to a diagnosis of celiac disease.
Szymanski has had to start over on his bike more than once. Among other motivations, two constant reminders: First, lots still to do in life. Second, it’s not forever. Photo courtesy of Steve Szymanski.
Cutting gluten made no difference. Szymanski arrived at UCHealth University of Colorado Hospital on the Anschutz Medical Campus (UCH) without a diagnosis. Szymanski’s wife Cyd estimates that they saw 15 doctors before meeting with UCHealth and CU School of Medicine internal-medicine physician Dr. Lisa Corbin. She referred Szymanski to gastrointestinal and other specialists, one of them being Dr. Kevin Deane, a CU School of Medicine and UCHealth colleague and rheumatologist.
The autoimmune-disease specialist ordered more tests. Deane noted high levels of protein in Szymanski’s urine – something previous tests had also found. He also ordered a blood test that looks for light-chain proteins. These queries would seem to have little to do with abdominal and back pain, but Deane’s experience as a rheumatologist had taught him to cast a wide net.
“Because our diseases are pretty rare, sometimes rheumatologists look for other things that mimic one of our diseases,” Deane said.
Stem-cell transplant
The light-chain protein test results convinced Deane that Szymanski would be best served by a hematologist. Before Deane even had the chance to meet Szymanski, he referred him to CU School of Medicine and UCHealth blood-cancer specialist Dr. Clay Smith. Smith soon diagnosed amyloidosis caused by multiple myeloma and coordinated a UCHealth care team including experts in cardiology, gastroenterology, infectious diseases and nephrology.
Amyloidosis, a tricky diagnosis, can be traced to Vietnam and exposure to Agent Orange
https://www.uchealth.org/today/amyloidosis-diagnosis-traced-to-agent-orange-exposure/
So, what is Agent Orange’s mechanism of long-term destruction? It is a stored toxin that does not leave and is not removed from the body. As it remains in the body it creates the conditions that induce chronic disease. Let’s take a look at what it can do.
Neurological System
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Parkinson disease and parkinsonianism¹
Peripheral neuropathy² ]
Stroke²
Mild cognitive impairment and dementiaUpper and Lower Respiratory Tract
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Idiopathic pulmonary fibrosis
Laryngeal cancer²
Lung cancer²Cardiovascular System
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Hypertension¹
Ischemic heart disease²
Hepatobiliary and Gastrointestinal SystemsLiver disease and cirrhosis
The components of Agent Orange have been shown to cause acute liver injury, and dioxin-related hepatotoxicity can lead to steatosis and cirrhosis.[11][75][76][77][78] However, there has not been a consistent association between exposure to the herbicide and these health outcomes.[1][12][13][79][80][81]
Renal System
Studies examining effects on renal function and rates of renal malignancies did not find evidence of an association with Agent Orange exposure.[59] However, some study results have suggested an association between chronic, high dioxin exposure in endemic populations with decreased eGFR and an increased incidence of chronic kidney disease.[82][83][84]
Hematologic System
1 Strong Evidence, 2 Limited or Suggestive Evidence:
AL amyloidosis²
Chronic lymphocytic leukemia¹
Hodgkin lymphoma¹
Non-Hodgkin lymphoma¹
Myeloproliferative neoplasms
Monoclonal gammopathy of undetermined significance (MGUS)¹
Multiple myeloma²Immunologic System
Rheumatoid arthritis [80][101][102][103]
Genitourinary System
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Prostate cancer² [59][63][105][106][107][108][109]
Urinary bladder cancer² [59][110][111][112][113]Endocrine System
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Type 2 diabetes¹,²
Hypothyroidism²
Thyroid cancerReproductive System
Reduced sperm quality [129][130][131]
Reduced female fertility [132][133][134]Developmental Adverse Effects
Congenital abnormalities and malformations
Congenital hypothyroidism
Congenital heart disease
Neurodevelopmental issuesOther Oncologic Conditions
1 Strong Evidence, 2 Limited or Suggestive Evidence:
Soft tissue sarcoma¹
Other malignancies
Agent Orange Toxicity
https://www.ncbi.nlm.nih.gov/books/NBK594243/
Tha parallels to pathological conditions induced by the Spike Protein are ubiquitous. But why? One key mechanism may be how both affect mitochondria.
Researchers with the University of Pennsylvania School of Veterinary Medicine have demonstrated the process by which the cancer-causing chemical dioxin attacks the cellular machinery, disrupts normal cellular function and ultimately promotes tumor progression.
The team identified for the first time that mitochondria, the cellular sub-units that convert oxygen and nutrients into cellular fuel, are the target of tetrachlorodibenzodioxin, or TCDD. The study showed that TCDD induces mitochondria-to-nucleus stress signaling, which in turn induces the expression of cell nucleus genes associated with tumor promotion and metastasis.
Agent Orange Chemical, Dioxin, Attacks the Mitochondria To Cause Cancer, Says Penn Research Team
https://penntoday.upenn.edu/news/agent-orange-chemical-dioxin-attacks-mitochondria-cause-cancer-says-penn-research-team
Now, let’s look at how the Spike Protein may, over time, induce similar effects to Agent Orange. Instead of being stored in the body, it is continually expressed via repeated exposures to the Spike Protein via SARS-CoV-2 infection or Spike Protein-based vaccination. For example, the Spike Protein has been found to be expressed some 180 days post vaccination.
It was hoped that resident and circulating immune cells attracted to the injection site make copies of the spike protein while the injected mRNA degrades within a few days. It was also originally estimated that recombinant spike proteins generated by mRNA vaccines would persist in the body for a few weeks. In reality, clinical studies now report that modified SARS-CoV-2 mRNA routinely persist up to a month from injection and can be detected in cardiac and skeletal muscle at sites of inflammation and fibrosis, while the recombinant spike protein may persist a little over half a year in blood.
Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination
https://bpspubs.onlinelibrary.wiley.com/doi/10.1002/prp2.1218
And it may be possible that being infected with COVID can cause continual expression of the Spike Protein as it has been found in Long COVID patients and those who had a “resolved” case of COVID.
SARS-CoV-2 components (S, spike subunit S1, and nucleocapsid [N] proteins) can remain in circulation and across various systems and tissues for a considerable time [40,41]. Indeed, SARS-CoV-2 components have been identified in the respiratory, cardiac, renal, reproductive, and central nervous systems (CNS), as well as in lymph nodes, muscles, the liver, and the gastrointestinal tract (GI) [27,42,43]. In a recent study analyzing almost 94,000 viral sequences to rule out reinfection cases, and from the follow-up of 381 individuals, it was observed that up to 0.5% of SARS-CoV-2 infections may become persistent for at least 60 days, usually with viral rebounds [44]. Individuals with viral persistence had a greater than 50% likelihood of developing long COVID, with 30% experiencing viral rebounds. Most cases of viral persistence were resolved in less than three months, although not all cases resulted in LC (only 9% did). Furthermore, in an autopsy study of 44 patients, the persistent presence of SARS-CoV-2 RNA was detected at various anatomical sites, including the brain, cervical spinal cord, and olfactory nerve, persisting between 31 and 230 days after the onset of symptoms [45,46].
SARS-CoV-2 Spike Protein and Long COVID—Part 1: Impact of Spike Protein in Pathophysiological Mechanisms of Long COVID Syndrome
https://pmc.ncbi.nlm.nih.gov/articles/PMC12115690/
As with HIV and other long-term conditions, the intial flu-like symptoms of COVID may be parallel to the initial flu-like symproms of HIV. Then, after continual expression/exposure to the spike protein, just like HIV, years or decades later serious medical consequences may emerge. This needs to be studied with great urgency as the evidence continues to mount that the above amyloidosis scenario associated with Agent Orange may occur, along with many other possible conditions, in those exposed to the Spike Protein. Of course, myriad more have been exposed to the Spike Protein than were ever exposed to Agent Orange. I will continue to work on understanding and solutions. Please have a blessed week.
I would like to thank the individual who made a generous PayPal donation over the weekend. Given the current inflationary climate, it is immensely appreciated.
We don't even need to hypothesize what the Spike can do; the entire United States housing stock is LOADED with PVC. To make dioxin (i.e. the most toxic part of Agent Orange), all you need to do is light that house on fire. EVERY SINGLE MODERN HOME is a deadlly toxin bomb just waiting to be activated.
I'm building a house now and while I have tried to avoid using PVC everywhere possible, it's literally impossible to avoid completely with what the industry makes available and with how the building codes are written and enforced.
I need more people elevating this concern to the highest levels of government (RFK jr); chlorinated plastics need to be banned with almost no exceptions. PVC + fire is more dangerous than DDT, asbestos, lead, mercury combined. There is NO chemical more toxic than dioxin/ TCDD.
Spike proteins can be broken down (with effort); I've been having to do this for the past few years now (due to my extreme sensitivity to the shedding) and I'm getting better at it every month using natural plant medicines. Dioxins have no antidote; it's nearly impossible to clear these things from our bodies. There's just no contest.
Please forward this to Robert F. Kennedy Jr. (HHS Secretary), Dr. Makary (Head of FDA) and Dr. Robert Malone ("expert" on mRNA, member of vaccine advisory committee). Perhaps if you highlight/emphasize that the experimental mRNA injections cause this amyloidogenesis , they will finally remove all mRNA injections from the market immediately (as should have been done on day one of RFK Jr. appointed and confirmed as HHS Secretary. I believe that Malone is actually in favor of developing the dangerous mRNA platform for vaccines and will not recommend pulling them off the market (I believe it is due to his ego (as he was involved in initial development of the mRNA technology), he cannot admit that it has been a complete failure and used in the COVID injections , caused a massive number of serious long-term injuries (including heart issues, blood clotting issues, cancers, aneurysms, strokes, dementia, other autoimmune disorders, miscarriages, stillbirths, post-partum hemorrhages) and potentially hundreds of thousands of deaths around the world. There may be many cases of long-COVID health issues that extend for many months but I believe that compared to the degree of serious adverse effects and deaths caused by the mRNA COVID in jections, your focus and emphasis should be on the inherent health risks caused by the mRNA injections! The reason so many physicians continue to deny that patients have been injured (or died) from the COVID mRNA injections is because they have been told that since the beginning of the administration of the mRNA injections, that any patients presenting with adverse effects and illnesses after receiving the mRNA injections are experiencing Long COVID!!!!! This is why patients are being denied an accurate diagnosis and receiving the necessary treatment and physicians continue to recommend that these patients (especially the elderly) continue to receive the COVID mRNA boosters on a regular basis!!!! Each COVID mRNA booster increases the patient's chances of developing more serious health issues and even death! So if you continue to present your clinical observations and analyses with reporting the adverse effects as Spike Protein due to Long COVID rather than the emphasis on the mRNA injections being far more likely to directly cause these adverse health effects (see Steve Kirsch's work, and Nicolas Hulscher and Dr. Peter McCullough's work that include numerous studies that prove that the mRNA injections have caused far more serious adverse effects and deaths than in the cases of Long COVID. We need to have your knowledge and expertise in this area participate in the clarion call to remove the mRNA injections from the market completely (they are not safe or effective for anyone in any age group or even immune-compromised, etc) and send your substack articles (hopefully with emphasis on the toxicity of the mRNA injections) to the Federal officials at HHS.