
Spike Protein Denervation: An Important, Undiscussed Possible Cause for Observed Sudden Cardiac Deaths
The Spike Protein induces denervation post mRNA vaccination and post infection (Long COVID).

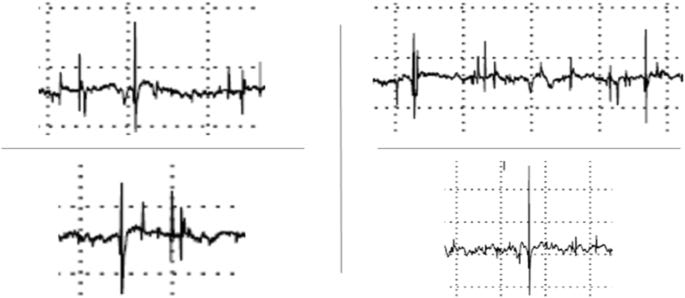
Fiber spontaneous activity (fibrillation potentials in right and left genioglossus muscle)
I have long maintained that Myocarditis alone cannot account for the dramatic increase in Sudden Cardiac Deaths since the appearance of COVID and its mRNA vaccines. I now submit proof that the Spike Protein induces denervation, which, of course, can have fatal consequences when the heart is involved. This finding may also explain why there are innumerable reports of buzzing and vibrating involved with COVID and Spike Protein exposure.
Let us start with the case of a 42-year-old male who had severe COVID pneumonia. This demonstrates denervation in the context of acute infection.
A complete neurophysiological examination showed denervation in the left hypoglossus nerve, without other nerves involvement (above). Electroneuromyography at 4 limbs showed mild amplitude reduction of sensitive and motor action potentials in all examined nerves (symmetrical and disto-proximal distribution) with mild denervation EMG pattern in arm proximal muscles. CSF analysis showed albumin-cytologic dissociation (52 mg/dl CSF protein, with 2 cells/mmc, normal glucose and cytology): negative was rRT-PCR for COVID-19 in CSF such as serum anti-ganglioside antibodies. Cerebral and cervical MRI was negative.
Selective cranial multineuritis in severe COVID-19 pneumonia: two cases and literature review
https://link.springer.com/article/10.1007/s10072-021-05087-4
Now, let us look at denervation in the context of Long COVID.
Study of nerve conduction velocities, somatosensory-evoked potentials and electromyography of the lower and upper extremities (17 April 2021) that report findings compatible with post-COVID mixed polyneuropathy, evidencing the presence of a moderate to severe sensory–motor polyneuropathic process, with a mixed pattern but one which was predominantly axonal, affecting the four extremities with greater expression in the lower extremities and predominance on the right; chronic partial denervation data were recorded in the four extremities.
Post-Coronavirus Disease 2019 Triggers the Appearance of Mixed Polyneuropathy and Brain Fog: A Case Report
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9149881/
Lastly, we find an example of denervation post mRNA vaccination.
Nerve conduction studies (NCSs) were performed 3 days after the second inoculation. These studies revealed that left radial compound muscle action potential (CMAP) was markedly reduced, compared to the right side. Sensory nerve action potential (SNAP) was also relatively reduced in the left radial nerve . Followup NCS also showed reduced CMAP, and needle electromyography showed acute denervation of the left extensor carpi radialis longus, extensor digitorum communis, and anconeus muscles 17 days after symptom initiation. Based on these results, left radial neuropathy in the axilla with demyelination and associated mild axonal injury were highly suspected.
Ipsilateral Radial Neuropathy after COVID-19 mRNA Vaccination in an Immunocompetent Young Man
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9520044/
Since the Spike Protein is the only viral protein expressed in mRNA vaccination, it is most certainly a causal factor.
Why I am so concerned is that, as this appears to be systemic (occurring in multiple locations), it can explain Sudden Cardiac Deaths. As the Spike Protein not only induces Myrocarditis, but also appears to mimic denervation associated with Ischemic Cardiomyopathy.
Relatively few studies have evaluated cause-specific mortality and most, including the primary analysis of the PAREPET trial, focused on SCA (Sudden Cardiac Arrest) versus death from all other causes. The present study extends our original report by providing novel information from a competing risks analysis. The competing risks methodology allows for the simultaneous assessment of the mutually exclusive components of cardiac mortality, namely SCA and NSCD (Nonsudden Cardiac Death). With regard to SCA, 3 of the variables remained the same as in the original multivariable analysis of SCA alone. These included greater extent of denervated myocardium, larger LVEDVI, and lack of angiotensin inhibition therapy. The competing risks analysis replaced an elevated creatinine with an elevated BNP. This change is consistent with a previous study that evaluated clinical, hemodynamic, and neurohormonal factors in patients with heart failure and found that BNP was the only independent variable associated with SCA. The factors we identified suggest that SCA risk is not only influenced by potential alterations in ventricular repolarization (because of regional sympathetic denervation) but also by ventricular remodeling (as reflected by elevated LVEDVI and prevented by angiotensin inhibition therapy) and chronic elevations in LV end-diastolic pressure (BNP). These factors would also tend to promote interstitial fibrosis, which would delay ventricular impulse conduction and increase the risk of reentry. They could also lead to stretch-induced arrhythmogenesis, which has been observed in an animal model of sudden death from chronic ischemia without infarction.
Denervated Myocardium Is Preferentially Associated With Sudden Cardiac Arrest in Ischemic Cardiomyopathy
https://www.ahajournals.org/doi/full/10.1161/CIRCIMAGING.117.006446
Please note the other Spike induced cardiac pathologies present in the above.
I will be researching this further. It is, however, that we begin a dialog immediately.
Thank you for your readership and your support.
Wow, Walter, I really admire your strength. You're still hacking at this jungle of shit.
It's like you're that crazy detective that still can put 2 and 2 together, while all the others just KNOW it's 5.
Thanks Walter, this relates to the Substack I'm preparing on autoimmune neurological disorders, I will cite your work.