Persistent Cardiac Conduction Dysfunction: New Evidence of SARS-CoV-2 Mimicking Radiation and Activation of HERVs
Activation of HERVs induces dsRNA immune response and mitochondrial damage.

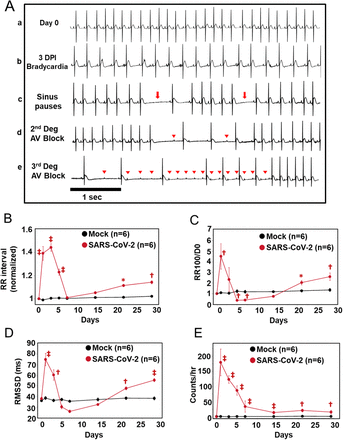
Effects of SARS-CoV-2 infection on cardiac electrophysiology in the hamster model.
Representative ECG recording showing normal baseline rhythm (a) and arrhythmias induced by SARS-CoV-2 infection including bradycardia (b), sinus pauses (c, arrows), 2nd degree AV block (d) and 3rd degree AV block (e). Arrowheads indicate p waves. Horizontal bar: 1 sec. (B-E) Analysis of ECGs from 0 to 28 dpi typically showed a triphasic pattern of SARS-CoV-2 effects on cardiac rhythm: an acute peak within 7 dpi, recovery to, or below, baseline, and a long-term effect developing between 7 dpi and 28 dpi. Mean RR interval (normalized to D0) (B), incidence of long sinus pauses (RR>meanRR+100ms; normalized to D0) (C), and RMSSD (D) peaked at 1-3 dpi, and returned to levels close to or lower than baseline, and then gradually increased to levels significantly higher than baseline at 21 and 28 dpi. The rate of AV Block events (E) peaked early and did not return to baseline level, remaining significantly higher than baseline between 7 and 28 dpi. Red symbols denoting p-values * p<0.05; † p<0.01; ‡ p<0.0001 on the figures compare mock vs. SARS-CoV2 infected groups. P-values comparing SARS-CoV-2 data from day 0 through day 28 are available in Supplementary table 4.
A preprint was published online January 8th which supports many of the mechanisms I have proposed for Spike Protein/SARS-CoV-2 pathology. From cell remodeling to Ca2+ conduction irregularities and ROS damage mimicking radiation. Perhaps the most interesting discovery is that, in the absence of viral RNA, the presence of dsRNA induced the same arrythmias as the virus itself.
The evidence gives a clear image that Sudden Cardiac Deaths may be attributable to more than just the observed cases of fulminant myocarditis. A picture is emerging of a persistent attack on the conduction system of the heart from early on in SARS-CoV-2 infection.
ECG analysis revealed that SARS-CoV-2 infection resulted in multiple types of cardiac arrhythmias linked to CCS dysfunction, including bradycardia, sinus pauses, and 2nd and 3rd degree atrioventricular (AV) block. The effects had a triphasic pattern: an early peak at 1-3 dpi, a recovery phase by 7 dpi, and arrhythmia redevelopment that persisted through 28 dpi. As early as 1 day after SARS-CoV-2 infection, marked bradycardia was observed.
Also, autonomic nervous system dysfunction.
Evidence of autonomic nervous system dysfunction was also observed. Heart rate variability analysis revealed that the root mean square of the successive RR differences (RMSSD) was significantly higher than baseline at 1 and 3 dpi and lower at 5 and 7 dpi (74.9 ± 5.7ms at 1 dpi; 60.3 ± 4.9ms at 3 dpi; 30.4±1.7ms at 5 dpi; 26.1 ± 1.4ms at 7 dpi vs. 38.1 ± 1.6ms at 0 dpi), suggesting increased parasympathetic activity followed by impaired vagal responses during the acute COVID phase.
Additionally, cardiac conduction system remodeling has been recorded.
We propose that the observed CCS remodeling and altered local crosstalk between myocytes and immune cells is responsible for impaired function.
What I object to in this study is that the authors state there is NO viral RNA present. However, they only tested for the N protein! To me, this is unconscionable.
To test whether SARS-CoV-2 was directly infecting the heart, we probed for viral nucleocapsid expression in whole heart and lung homogenates by western blot or by immunofluorescence in lung or myocardial tissue slices. Western blot showed no detectable viral nucleocapsid protein in myocardial lysates at 4 dpi, while two bands were readily detected in infected lungs. Widespread nucleocapsid expression was evident in the lung at 4 dpi but was absent in the myocardium.
I am quite certain the results of viral presence would be quite different had they troubled themselves to test for the Spike.
What I find most interesting about this paper, is that the authors proceeded to give an RNA mimetic, polyinosinic:polycytidylic acid (PIC), which induced precisely the same arrhythmic events that the infected animals experienced.
Interestingly, the arrhythmia phenotype was reproduced by cardiac injection of PIC in the absence of virus, indicating that innate immune activation was sufficient to drive the response. PIC also strongly induced cytokine secretion and robust interferon signaling in hearts, human iPSC-derived cardiomyocytes (hiPSC-CMs), and engineered heart tissues, accompanied by alterations in electrical and Ca2+ handling properties. Importantly, the pulmonary and cardiac effects of COVID-19 were blunted by in vivo inhibition of JAK/STAT signaling or by a mitochondrially-targeted antioxidant.
Innate Immune Activation and Mitochondrial ROS Invoke Persistent Cardiac Conduction System Dysfunction after COVID-19
https://www.biorxiv.org/content/10.1101/2024.01.05.574280v1.full
This relates directly to my recent findings. Activation of Human Endogenous Retroviruses (HERVs) cause the expression of dsRNA, which the Spike Protein activates.
Endogenous sources of dsRNA
Endogenous retroviruses
(ERVs). endogenous viral elements in the genome that closely resemble and can be derived from retroviruses. These elements constitute up to 8% of the human genome.
Long interspersed nuclear elements
(LINEs). a group of retrotransposons that are not long terminal repeats. LINEs constitute ~21% of the human genome. They are transcribed into mRNA and translated into a protein that acts as a reverse transcriptase, which makes a DNA copy of the LINE RNA, which then can be integrated into the genome at a new site.
Cellular origins of dsRNA, their recognition and consequences
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8969093/
There is some hope in all of this. The arrhythmic effects were blunted by the use of an mitochondrially-targeted antioxidant.
My concern is that continued expression of dsRNA will eventually degrade the CCS to such an extent that, indeed, the heart simply is unable to work. We need data. We need to study everyone. From those who have had Long COVID for years, to those who had asymptomatic infection. Also, this invokes the need to fully understand if the Spike (or any part of SARS-CoV2) is being retrotranscribed.
Thank you, as always, for your readership and support.
Thank you Walter. Amazing work. Peace.
Like I keep saying.. as I have for the last 17 months.. mitochondrial function is all important... why? Because heart tissue has 10,000 in each myocyte(heart cell) as opposed to 2,000 in muscle...and a poorly functioning cell will produce poor cardiac function.
If you have this problem the best solution is Astaxanthin much more potent than C0q10 vitamin E and C... and Tocotrienols... which repair nerves.. which improve electrical pathways...
Lastly remove the damaged mitochondria through pomegranate extract or juice.. this causes mitophagy which only removes dead dedunct and misfolded mitochondria .. so new can form... otherwise stay crippled.