

Of Spike Proteins and Rabies: How the Spike Protein Mimics Rabies Axonal Degeneration and May Explain Many Sudden Deaths
Just as in Rabies, the Spike Protein invades the CNS via Retrograde Transport.

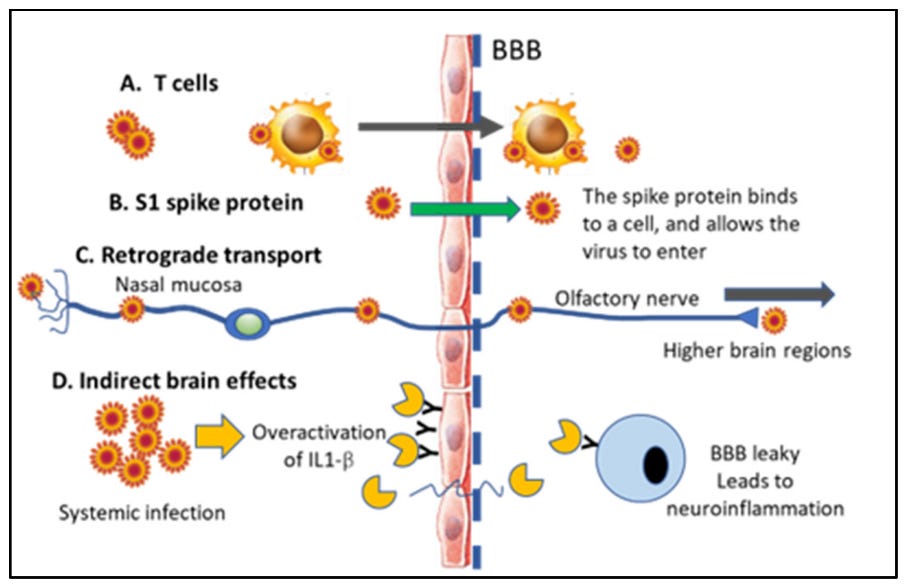
Direct and indirect effects of SARS-CoV-2 virus on the brain and mode of entry into the CNS. (A) The virus can enter together with T cells since an infection can alter the BBB permeability. (B) The SARS-CoV-2 Spike 1 protein can attach to endothelial cells and insert the virus into the cells of the BBB. (C) The virus attacks the nasal mucosa and can be transported retrogradely via olfactory nerves either with direct retrograde transport or via exosomes into the CNS. The same retrograde transport of viral particles has also been proposed in other cranial nerves (trigeminal, facial, and vagal nerves). (D) Indirect entry of the SARS-CoV-2 virus into brain tissue may be caused by overactivation of the IL1-β inflammatory system in the body after infection, leading to elevated IL-1β and other proinflammatory cytokines in the blood. IL-1β has receptors on endothelial cells, and binding to its receptors causes re-conformation of the BBB, allowing both blood cells and cytokines to enter the brain. IL1-β then binds to its receptors on glial cells and neurons within the CNS, leading to progressive neuroinflammation and neuronal loss. Since brain pathology is caused by blood-based cytokines and not the virus itself, this leads to an indirect effect on the brain via systemic infection. Small solar-shaped figure represents the virus and yellow shape in D represents IL-1β. “Y” in D represents IL-1β receptor.
Rabies has an interesting way of killing you. It causes your neurons to self-destruct. It enters the nervous system by walking backwards (retrograde) from the initial bite, through the nerves connected to the local muscles. The axons of the neurons are destroyed this way by the virus' induction of the loss of NAD.
Neurotropic viral infections continue to pose a serious threat to human and animal wellbeing. Host responses combatting the invading virus in these infections often cause irreversible damage to the nervous system, resulting in poor prognosis. Rabies is the most lethal neurotropic virus, which specifically infects neurons and spreads through the host nervous system by retrograde axonal transport. The key pathogenic mechanisms associated with rabies infection and axonal transmission in neurons remains unclear. Here we studied the pathogenesis of different field isolates of lyssavirus including rabies using ex-vivo model systems generated with mouse primary neurons derived from the peripheral and central nervous systems. In this study, we show that neurons activate selective and compartmentalized degeneration of their axons and dendrites in response to infection with different field strains of lyssavirus. We further show that this axonal degeneration is mediated by the loss of NAD and calpain-mediated digestion of key structural proteins such as MAP2 and neurofilament.
Novel role of SARM1 mediated axonal degeneration in the pathogenesis of rabies
https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1008343
Now, the way this relates to the Spike Protein is equally fascinating.
I first noticed this report of axonal damage markers in those with COVID.
Previous studies have pointed out several alterations in the levels of neuronal cerebrospinal (CSF) and glial cells (neuroglia). Also, changes in plasma biomarkers of COVID-19 patients with neurological symptoms were observed. For instance, changes in neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP) levels were found in COVID-19 patients with neurological manifestations. These studies documented evidence to support plasma NfL as a marker for neuroaxonal damage and GFAP as a marker for astrocytic activation/injury. Total tau (T-tau) protein has been considered to be another marker for axonal damage and neuronal degeneration in COVID-19 patients.
Are plasma levels of axonal damage and neuronal degeneration makers altered in COVID-19 patients without major neurological manifestations?
https://www.news-medical.net/news/20230203/Are-plasma-levels-of-axonal-damage-and-neuronal-degeneration-makers-altered-in-COVID-19-patients-without-major-neurological-manifestations.aspx
Then, after further research, I discovered that the Spike Protein indeed infects the CNS in the very same way Rabies does, by retrograde transport.
Let's begin by looking at the Spike Protein in another lethal Coronavirus, Mouse Hepatitis Virus.
Mouse hepatitis virus (MHV; murine coronavirus) causes meningoencephalitis, myelitis, and optic neuritis followed by axonal loss and demyelination. This murine virus is used as a commonmodeltostudyacuteandchronicvirus-induceddemyelination in the central nervous system. Studies with recombinant MHV strains that differ in the gene encoding the spike protein have demonstrated that the spike has a role in MHV pathogenesis and retrograde axonal transport.
Oneproline deletion in the fusion peptide of neurotropic mousehepatitis virus (MHV) restricts retrograde axonal transport and neurodegeneration
https://www.jbc.org/article/S0021-9258(17)48196-8/pdf
And so, the same is likely true for SARS-CoV-2 and its Spike Protein.
Viral penetration into the central nervous system through peripheral fibers is a multi-step process. In order to reach neuronal soma from the periphery, the virus needs to exploit the retrograde axonal transport machinery. SARS-CoV-2 uses ACE2-mediated endocytotic pathway for internalization and intracellular transport, and in the case of SARS-CoV-1 infection, endosomes containing virion/ACE2 complexes are trafficked to the perinuclear area (Wang et al., 2008). The virus might use this intrinsic clathrin-independent intracellular ACE2 endocytic transport to reach the perikaryon. However, for a successful further invasion, it would also need to be able to cross synaptic membranes. Another beta-coronavirus was shown to be capable of trans-synaptic propagation by presynaptic exocytosis and postsynaptic endocytosis (Li et al., 2013), which suggests that SARS-CoV-2 could use the same mechanism.
SARS-CoV-2 Dissemination Through Peripheral Nerves Explains Multiple Organ Injury
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7419602/
Yet, in order to mimic Rabies' axonal degeneration, there is one component that needs to be present. The depletion of NAD. This is, in fact, the case.
Many acute COVID-19 convalescents experience a persistent sequelae of infection, called post-acute COVID-19 syndrome (PACS). With incidence ranging between 31% and 69%, PACS is becoming increasingly acknowledged as a new disease state in the context of SARS-CoV-2 infection. As SARS-CoV-2 infection can affect several organ systems to varying degrees and durations, the cellular and molecular abnormalities contributing to PACS pathogenesis remain unclear. Despite our limited understanding of how SARS-CoV-2 infection promotes this persistent disease state, mitochondrial dysfunction has been increasingly recognized as a contributing factor to acute SARS-CoV-2 infection and, more recently, to PACS pathogenesis. The biological mechanisms contributing to this phenomena have not been well established in previous literature; however, in this review, we summarize the evidence that NAD+ metabolome disruption and subsequent mitochondrial dysfunction following SARS-CoV-2 genome integration may contribute to PACS biological pathogenesis. We also briefly examine the coordinated and complex relationship between increased oxidative stress, inflammation, and mitochondrial dysfunction and speculate as to how SARS-CoV-2-mediated NAD+ depletion may be causing these abnormalities in PACS.
Rationale for Nicotinamide Adenine Dinucleotide (NAD+) Metabolome Disruption as a Pathogenic Mechanism of Post-Acute COVID-19 Syndrome
https://journals.sagepub.com/doi/10.1177/2632010X221106986
When the pieces of the puzzle are finally put together, we find a very logical and convincing argument that many of the sudden deaths which cannot be attributed to myocarditis may indeed be due to the Spike Protein's (and SARS-CoV-2's) ability to destroy axons.
In the SAH group, histopathologically, severe anterior spinal artery (ASA) and arteriae nervorum vasospasm, axonal and neuronal degeneration, and neuronal apoptosis were observed. Vasospasm of ASA did not occur in the SS and control groups. There was a statistically significant increase in the degenerated neuron density in the SAH group as compared to the control and SS groups (P < 0.05). Cardiorespiratory disturbances, arrest, and lung edema more commonly developed in animals in the SAH group.
Sudden death and cervical spine: A new contribution to pathogenesis for sudden death in critical care unit from subarachnoid hemorrhage; first report – An experimental study
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5324357/
Cardiac lesions produced by central nervous system stimulation are morphologically indistinguishable from stress and catecholamine-induced cardiac damage. Back in 1963, Melville and colleagues51 produced bradycardia and myocardial necrosis in cats by stimulation of the anterior hypothalamus. Later on, Kannan and collaborators52 in 1989 induced an increase in blood pressure (BP) and renal sympathetic outflow in conscious rats by bilateral electrical stimulation of the paraventricular nucleus (PVN) of the hypothalamus or by microinjecting L-glutamate, an excitatory amino acid neurotransmitter, into the PVN. Morphological studies complemented functional studies and provided evidence of direct PVN axonal connections, from the parvocellular part to the respiratory, pre-Bötzinger complex, vasomotor and cardiac neurons in the rostro-ventro-lateral medulla and preganglionic neurons in the inter-medio-lateral column of the spinal cord.
Sudden death: Neurogenic causes, prediction and prevention
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5724572/
This preliminary work broadly outlines the mechanisms which may explain many of the very premature sudden deaths being observed. I have never accepted the premise that Spike Protein induced Myocarditis is the only mechanism at work causing these deaths. That being said, of course those deaths are of equal concern.
The more we study SARS-CoV-2, the more we discover that it appears to be an immense eminence grise in the body driving it, inexorably, to one demise or another. As I have stated from Day One: The Spike Protein is a Swiss Army Knife of death.
Thank you for your readership, dialog and support. We will continue to learn and to find solutions to manange, and hopefully eradicate, this malevolent scourge.
This is exactly what my father died from last Saturday, the 16th, a subarachnoid hemorrhage (SAH). 6 Covid shots later, he received from the VA, after I told them to STOP giving him shots 3 years ago, they continued. Horrific what they have done.
Thank you Walter. HIV does the same, via gp120.
Retrograde and anterograde transport of HIV protein gp120 in the nervous system
Farid Ahmed et al. Brain Behav Immun. 2009 Mar.
https://pubmed.ncbi.nlm.nih.gov/19111924/
Post-vax brain fog hypothesis:
https://doorlesscarp953.substack.com/p/pathophysiology-of-spike-protein