

LONG COVID (PASC) SLEEP DISORDERS AND SPED – THE MICROVASCULAR ETIOLOGY
Spike Protein induced Endothelial Dysfunction as cause of observed Long COVID sleep disturbances

Please see my previous posts for an explanation of how the Spike Protein of SARS-CoV-2 is inducing systemic endothelial damage.
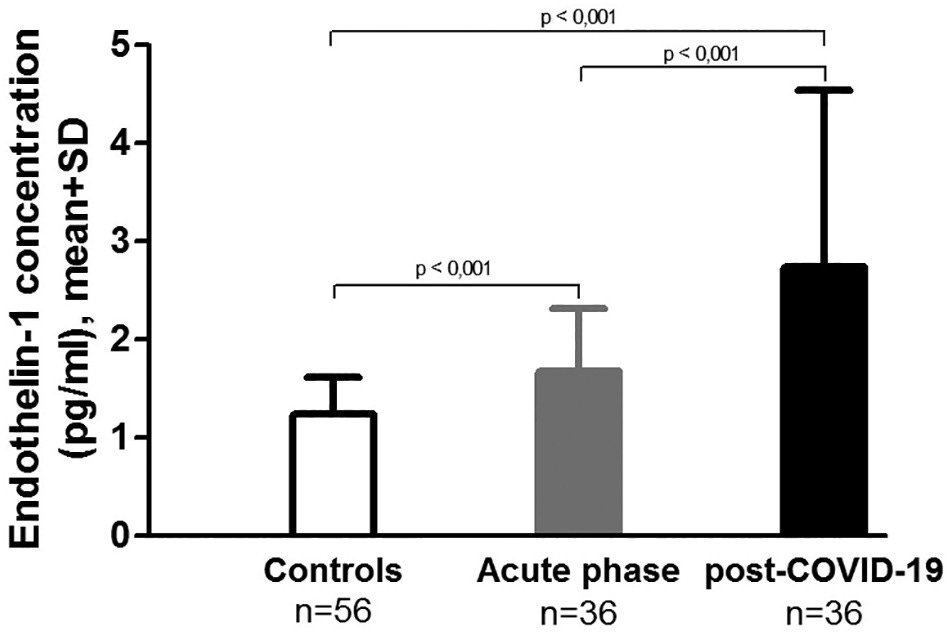
A paper published earlier this year (January 2022) found that those who have been infected with SARS-CoV-2 have elevated endothelin-1 levels, even three months after infection. The paper concluded that:
Based on this unique design, we found evidence of sustained endothelial cell activation, coagulation activation and inflammation. However, these changes did not coincide with macrovascular dysfunction, 3 months after acute COVID-19.
Yet, this has never been my major concern with COVID, Long COVID and the virus’ associated Spike Protein. My point has always been, and still is, that it is MICROVASCULAR damage which is the major, long term and cumulative concern.
Indeed, the paper ends with:
Future studies should pursue if high ET-1 levels as a marker of microvascular dysfunction play a role in long-term COVID complications.
I believe all readers know where I stand regarding these implications.
Sustained inflammation, coagulation activation and elevated endothelin-1 levels without macrovascular dysfunction at 3 months after COVID-19
https://www.sciencedirect.com/science/article/pii/S0049384821005491
To that point, I would like to address the sleep disturbances that are being report post COVID infection and in Long COVID. I believe that these disturbances are due to the cerebral microvascular endothelial damage caused by the virus, and in particular, its Spike Protein.
While the physiological underpinnings of the sleep and CVD relationship are not yet well defined, one plausible mechanism may be endothelial dysfunction, which is found in the early stages of atherosclerosis (Wolk et al.,2005). Circulating markers of endothelial cell activation and damage (e.g. von Willebrand factor, endothelin-1) are increased among patients with obstructive sleep apnea (OSA) compared to healthy controls(Phillips et al.,1999;Zamarrón-Sanz et al.,2006;El Solh et al.,2008) and among relatively healthy adults with increased sleep disturbance according to both self-reports (von Känel et al.,2010) and polysomnography-derived indices of sleep (e.g., latency in rapid eye movement or REM sleep)(Mills et al.,2007;von Känel et al.,2007;von Känel et al.,2010).
In addition, the Spike Protein’s upregulation of IL-6 I believe also plays a role in the sleep disturbances and, of course, the observed endothelial damage.
Systemic low-grade inflammation that is predictive of CVD might be another important mechanism linking REM sleep to endothelial dysfunction. Inflammatory processes contribute to and also are affected by endothelial dysfunction (Trepels et al.,2006). Greater REM latency has been associated with elevated plasma levels of the proinflammatory cytokine interleukin(IL)-6 (Mills et al.,2007). Subcutaneous administration of low-dose recombinant IL-6 was found to decrease REM sleep (Späth-Schwalbe et al.,1998).
Endothelial Function and Sleep: Associations of Flow-Mediated Dilation With Perceived Sleep Quality and Rapid Eye Movement (REM) Sleep
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3947135/
This also offers explanation as to why those who have Obstructive Sleep Apnea (OSA) are at a significantly higher risk for severe and fatal COVID, but not for contracting it.
Multiple logistic regression analysis showed that severe OSA was associated with increased odds of microvascular obstruction (odds ratio (OR), 5.10; 95% confidence interval (CI),1.61–16.2; p = 0.006). Mild and moderate OSA were also associated with increased odds of microvascular obstruction (mild OSA: OR, 2.88; 95% CI, 1.19–7.00; p = 0.019 and moderate OSA: OR, 3.79; 95% CI, 1.43–10.1; p = 0.008).
Severe obstructive sleep apnea is associated with coronary microvascular dysfunction and obstruction in patients with ST-elevation myocardial infarction
https://academic.oup.com/ehjacc/article/10/6/645/6145517
Risk for contracting COVID-19 was the same for patients with OSA and those without OSA. In contrast, among COVID-19 positive patients, OSA was associated with higher risk for hospitalisation. Our findings are in line with earlier works and suggest OSA as an independent risk factor for severe COVID-19.
Sleep apnoea is a risk factor for severe COVID-19
https://bmjopenrespres.bmj.com/content/8/1/e000845
I believe I have satisfactorily explained WHY those who have OSA are at increased risk for COVID.
Because of and independent of these findings, I believe it is critical to evaluate Endothelin-1 levels at monthly intervals post COVID vaccination.
This is additional evidence that THE VAST MAJORITY of COVID and Long COVID pathology is caused by Spike Protein Endothelial Disease (SPED).
Spooky as per usual. Thanks for being brutally honest.
Without this work, there can be no advance in actually treating the fucking thing.
And, yes it is also connected to UVB!
“UVB radiation generates sunburn pain and affects skin by activating epidermal TRPV4 ion channels and triggering endothelin-1 signaling”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752269/