

Friday Hope: Finerenone: Preventing Endothelial Dysfunction, Inflammation and Fibrosis
This mineralocorticoid receptor antagonist (MRA) may prove highly effective in treating Long COVID and in preventing Spike Protein Endothelial Disease and sequelae.

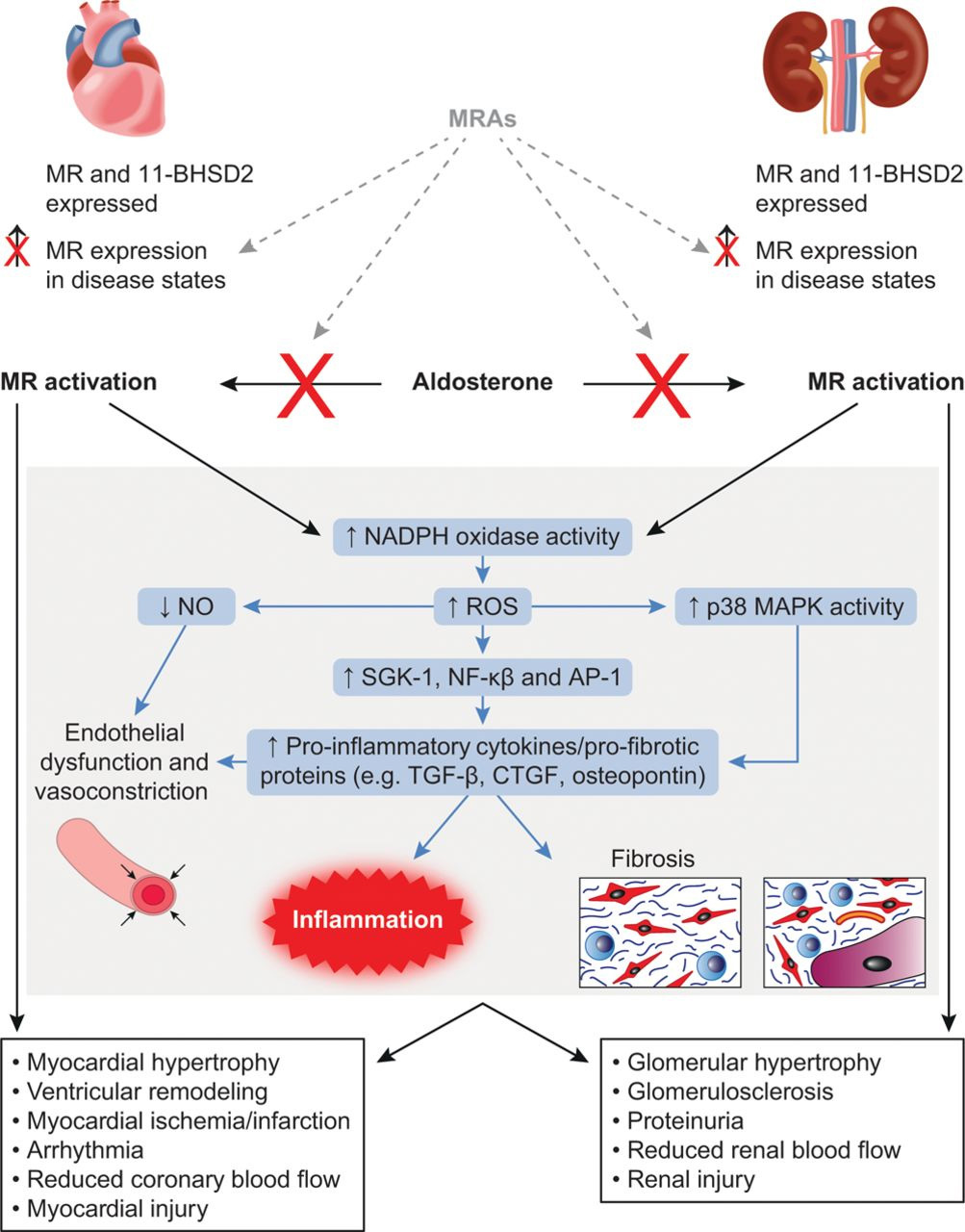
The direct deleterious effects of aldosterone/MR activation in the heart and kidneys and the common pathophysiological mechanisms involved. The benefits of MRAs in interrupting these pathways are also illustrated. 11-BHSD2 indicates 11β-hydroxysteroid dehydrogenase type 2; AP-1, activator protein-1; CTGF, connective tissue growth factor; NADPH oxidase, nicotinamide adenine dinucleotide phosphate-oxidase; MAPK, mitogen-activated protein kinase; MR, mineralocorticoid receptor; MRA, mineralocorticoid receptor antagonist; NF-κB, nuclear factor-κB; NO, nitric oxide; ROS, reactive oxygen species; SGK-1, serum- and glucocorticoid-induced protein kinase-1; and TGF-β, transforming growth factor-β.
It has been shown that the Spike Protein of SARS-CoV-2, through either infection or transfection, can cause kidney (multiple-organ) and endothelial damage.
According to recent studies, the SARS-CoV-2 spike protein found in vaccines may lead to kidney damage, either directly or indirectly (Figure 2). These studies have shown that certain tissue antigens, including transglutaminase 3, antiextraction nuclear antigen and thyroid peroxidase, can strongly react with SARS-CoV-2 antibodies.147 COVID-19 vaccines activate antigen-presenting cells (APCs), which, upon receiving a second vaccination, trigger robust CD4+ T-cell and CD8+ T-cell responses. This process results in the release of significant amounts of inflammatory cytokines (IFN-c, TNF-α, IL-2, IFN-γ and TNF), which can promote a cytokine storm and lead to damage to renal tissue.148,149 The receptor-binding domain (RBD) of the SARS-CoV-2 spike protein (S) has the ability to bind to natural antibodies in the body, which can lead to the formation of circulating immune complexes and their deposition in the glomeruli.150
It is currently speculated that COVID-19 vaccines, which target the spike protein as an immunogenic target, may also activate the complement system and lead to endothelial damage.
New insights into kidney disease after COVID-19 infection and vaccination: histopathological and clinical findings
https://academic.oup.com/qjmed/article/117/5/317/7218935
Several mechanisms are discussed above explaining how the Spike Protein may induce kidney and endothelial damage. However, there is one mechanism which is not mentioned. This is the mechanism of mineralocorticoid receptor activation. Please note that we will be discussing activation in not only the kidney, but also the heart, endothelium and immune system.
What is mineralocorticoid receptor (MR) activation?
MR expression has been demonstrated in vivo in vascular endothelial cells and vascular smooth muscle cells of interlobar arteries in mouse kidneys and ex vivo in cultured podocytes, mesangial cells, and renal fibroblasts.3 The MR is also expressed in multiple cell types in the heart, including cardiomyocytes, coronary endothelial and vascular smooth muscle cells, fibroblasts, and inflammatory cells, such as macrophages.5
Aldosterone and the glucocorticoid cortisol bind to the MR with similar affinities. Plasma concentrations of glucocorticoids are 100- to 1000-fold higher than those of aldosterone. Overstimulation of the MR is prevented by the coexpression of 11β-hydroxysteroid dehydrogenase type 2 (11-BHSD2). This enzyme converts cortisol into cortisone, which has a lower affinity for the MR. 11-BHSD2 activity has been demonstrated in both the kidneys and heart;6,7 however, expression of 11-BHSD2 varies in different cell types, with some cells, such as cardiomyocytes, having very low levels of 11-BHSD2. There is not yet consensus on whether aldosterone or cortisol activates the MR in these cells, but direct effects of aldosterone have still been observed, suggesting mechanisms yet to be determined fully may operate to allow the binding of aldosterone to the MR.8,9
Once aldosterone binds to the MR, the hormone–receptor complex dimerizes, migrates into the nucleus, and binds to a specific DNA sequence, triggering the transcription of target genes. It takes ≈1 hour for the classic genomic action of aldosterone to start to have a biological effect, with complete changes in gene expression not apparent for hours or days.10 A second, more rapid, nongenomic pathway, the effects of which are short-lived, has also been described, although the physiological and clinical relevance of this pathway remains to be established.11,12
The principal functional role of the MR in normal kidneys is to control sodium reabsorption and potassium secretion.3 The function of the MR in the healthy heart is not fully understood, but may include regulation of cardiomyocyte growth and cardiac electrophysiology.6,13
Mineralocorticoid Receptor Activation and Mineralocorticoid Receptor Antagonist Treatment in Cardiac and Renal Diseases
https://www.ahajournals.org/doi/10.1161/hypertensionaha.114.04488
In endothelial cells, aldosterone promotes oxidative injury and endothelial disfunction [19,20] as MR activation is involved in vascular calcification and fibrosis, stiffness, and inflammation [21]. Furthermore, the activation of mineralocorticoid receptors (MR) has been found to have additional pathological effects on the immune system and pro-inflammatory cells. This includes the stimulation of the infiltration of pro-inflammatory M1 macrophages as opposed to M2 macrophages, increased proliferation of fibroblasts, the production of molecules that promote fibrosis [22], and a reduction in nitric oxide levels due to the influence of MR on the expression of the epithelial sodium channel in the endothelium [23].
Finerenone: Questions and Answers—The Four Fundamental Arguments on the New-Born Promising Non-Steroidal Mineralocorticoid Receptor Antagonist
https://pmc.ncbi.nlm.nih.gov/articles/PMC10299719/
So, why look at Finerenone as a possible therapeutic for Long COVID/Spike Protein exposure? Because the Spike Protein activates mineralcorticoid receptors!
Vascular endothelial cells activation and dysfunction mediate inflammation and abnormal coagulation in COVID-19 patients. Mineralocorticoid receptor (MR) signaling and its downstream target Galectin-3 (Gal-3) are known to mediate cardiovascular inflammation and might be involved in the pathogenesis of COVID-19 complications. Accordingly, we aimed to investigate the potential beneficial effects of MR antagonism and Gal-3 inhibition on the inflammatory response induced by SARS-CoV-2 Spike protein in human aortic endothelial cells (HAECs). Methods: HAECs were treated with recombinant SARS-COV2 Spike (S) protein. MR antagonists (namely spironolactone and eplerenone) or the Gal-3 inhibitor G3P-01 were supplemented before and after S protein challenge. HAECs supernatants were assessed by ELISA or Western blotting. Results: HAECs treated with recombinant S protein resulted in enhanced secretion of inflammatory molecules (interleukin-6, monocyte chemoattractant protein-1, interleukin-18, interleukin-27, and interferon-γ) as well as in the thrombosis marker plasminogen activator inhibitor (PAI)-1. This was prevented and reversed by both MR antagonists and G3P-01. Conclusions: These findings indicate that MR/Gal-3 pathway blockade could be a promising option to reduce endothelial inflammation in SARS-CoV-2 infection.
Beneficial Effects of Mineralocorticoid Receptor Pathway Blockade against Endothelial Inflammation Induced by SARS-CoV-2 Spike Protein
https://pmc.ncbi.nlm.nih.gov/articles/PMC8228852/
It is my hope that clinicians will evaluate these findings and consider Finerenone in the treatment of their patients suffering from Long COVID/Spike Protein disease/injury. Please remember this is a work of medical research and not medical advice. Always consult your Primary Care Provider before using any medication or supplement.
We need clinical trials, clearly. I am quite optimistic that Finerenone may become a very prominent, effective player in treating those suffering from Long COVID/Spike Protein disease/injury. It is very cold here in northern Vermont. I look forward to keeping warm with a good game of chess tomorrow. Thank you for your gracious and generous support, readership and dialogue. I will continue to search for answers.
My coworker ended up with kidney failure after the second jab. Her nephrologist said the COVID vaccine was the cause.
Subcellular melatonin modulates the inflammatory response, and something we can all tap into (without supplements) during the winter: https://romanshapoval.substack.com/p/oralmelatonin