

Friday Hope: Aspirin: Inhibiting NLRP3 Inflammasome and Protecting Against COVID/Spike Endothelial Injury
Aspirin has also been shown to have significant prophylactic effects if taken before COVID infection.

Given all the recent evidence that the Spike Protein induces Cardiac Fibrosis by activating the NLRP3 inflammasome, I began a search for therapeutics to ameliorate this effect. In Aspirin not only have we found a safe, readily available therapeutic which inhibits the NLRP3 inflammasome, but also protects against endothelial damage caused by COVID infection and the Spike Protein.
First, generally speaking, Aspirin appears to be tailor-made for protecting the endothelium against Spike Protein injury and damage. The Spike Protein is a “lipopolysaccharide delivery system” in and of itself, causing the aforementioned damage.
Accumulating evidence indicates a potential role for bacterial lipopolysaccharide (LPS) in the overactivation of the immune response during SARS-CoV-2 infection. LPS is recognized by Toll-like receptor 4, mediating proinflammatory effects. We previously reported that LPS directly interacts with SARS-CoV-2 spike (S) protein and enhances proinflammatory activities. Using native gel electrophoresis and hydrogen-deuterium exchange mass spectrometry, we showed that LPS binds to multiple hydrophobic pockets spanning both the S1 and S2 subunits of the S protein. Molecular simulations validated by a microscale thermophoresis binding assay revealed that LPS binds to the S2 pocket with a lower affinity compared to S1, suggesting a role as an intermediate in LPS transfer. Congruently, nuclear factor-kappa B (NF-κB) activation in monocytic THP-1 cells is strongly boosted by S2. Using NF-κB reporter mice followed by bioimaging, a boosting effect was observed for both S1 and S2, with the former potentially facilitated by proteolysis. The Omicron S variant binds to LPS, but with reduced affinity and LPS boosting in vitro and in vivo. Taken together, the data provide a molecular mechanism by which S protein augments LPS-mediated hyperinflammation.
SARS-CoV-2 spike protein as a bacterial lipopolysaccharide delivery system in an overzealous inflammatory cascade
https://pubmed.ncbi.nlm.nih.gov/36240490/
Now, we turn to Aspirin to find that it is an ideal therapeutic for this phenomenon. Also, it inhibits the NLRP3 inflammasome activation which is causative in Spike Protein-related Cardiac Fibrosis.
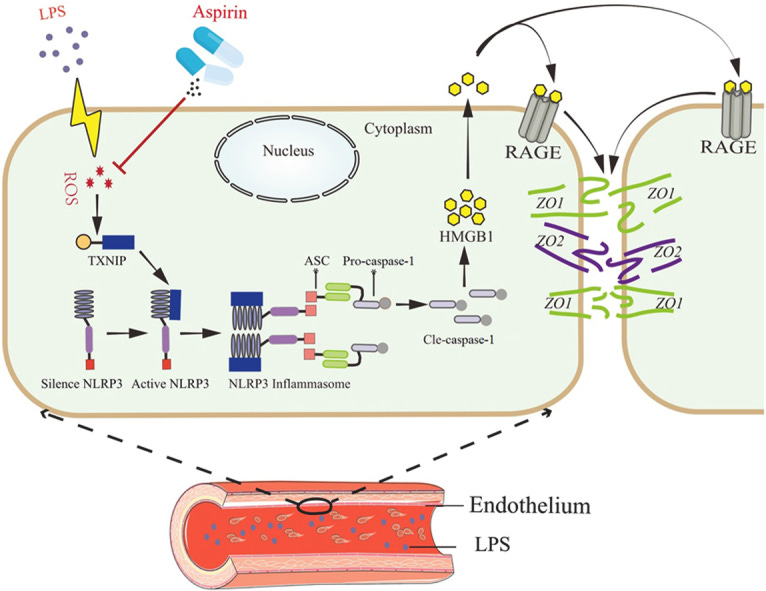
In this study, we demonstrated a novel role of aspirin in LPS-induced inter-endothelial junction disruption for the first time. Our findings showed that aspirin protected the expression of inter-endothelial junction proteins including zonula occludens-1 (ZO-1) and zonula occludens-2 (ZO-2) by inhibiting NLRP3 inflammasome pathway. The binding of LPS with TLR4 increases ROS release and NLRP3 inflammasome activation, leading to pyroptosis and tissue damages17., 18.. NLRP3 inflammasome activation is mediated by thioredoxin-interacting protein (TXNIP)19. And recent work demonstrated that NLRP3 inflammasome induced the release of high mobility group box 1 (HMGB1) to cause endothelial dysfunction20., 21.. In addition, aspirin was proved to play a key role in interdicting redox signaling and inhibiting NLRP3 inflammasome, thereby reduce endothelial injury and vascular endothelial dysfunction. Our study implicates the clinical potential of aspirin for the prevention of chronic vasculopathy on the early stage.
Aspirin alleviates endothelial gap junction dysfunction through inhibition of NLRP3 inflammasome activation in LPS-induced vascular injury
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6664043/
Yet, there is even more good news regarding our dear friend Aspirin. It is shown to reduce mortality for those suffering from COVID infection.
The results showed that aspirin use was associated with a reduction in COVID-19 mortality (adjusted RR 0.69; 95% CI 0.50–0.95; P < 0.001). Subgroup analysis found that the low-dose group was associated with a reduced COVID-19 mortality (adjusted RR 0.64; 95% CI 0.48–0.85; P < 0.01). Aspirin use was associated with reduced COVID-19 mortality in Europe and America (crude RR 0.71; 95% CI 0.52–0.98; P = 0.04), and results from cohort studies suggested that aspirin use was a protective factor for COVID-19 mortality (adjusted RR 0.73; 95% CI 0.52–0.99; P = 0.04). Meanwhile, aspirin use was not associated with bleeding risk (crude RR 1.22; 95% CI 0.80–1.87; P = 0.96).
Does aspirin have an effect on risk of death in patients with COVID-19? A meta-analysis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9217117/
To conclude this post, I will add perhaps the icing on the cake. Aspirin as prophylaxis that was continued during hospitalization had a profound beneficial effect as part of an antiplatelet regimen.
Moreover, the favourable effect was highly noticeable in this subgroup where acetylsalicylic acid was continued during hospitalization with reduction of in-hospital: 19% vs. 43%, 0.31 (0.15–0.67), 3-month: 30% vs. 54%, 044 (0.26–0.75) and 6-month mortality: 33% vs. 54%, 0.49 (0.29–0.82) when confronted with the subgroup who had acetylsalicylic acid suspension during hospitalization. The AP may have a beneficial impact on hospital course and mortality in COVID-19 and shouldn’t be discontinued, especially in high-risk patients.
Antiplatelet therapy prior to COVID-19 infection impacts on patients mortality: a propensity score-matched cohort study
https://www.nature.com/articles/s41598-024-55407-9
Please remember that the above is a work of medical research and not medical advice. Do not begin an aspirin regimen or use aspirin, or any other medication or supplement, without consulting your Primary Care Provider.
Thank you! Your support is the wind beneath my wings. I do read every comment, and many have been springboards for additional findings and therapeutic discoveries. It is a sultry late summer day here in Vermont. Looking forward to the cool, crystalline days of Autumn fast approaching. Please have a blessed and joyous weekend.
No wonder the Gov downgraded Aspirin recommendations during the pandemic
Walter, you are a wealth of timely and relevant knowledge. Thanks for working so hard and for sharing your findings. I look forward to every article. You really dig into the nuance and sort through the weeds. We appreciate you!