

An Urgent Warning: The Spike Protein Expressed On The Cell Surface Causes “Transplant Rejection” Of The Entire Body - Long COVID
Every Organ Expressing Spike Is Attacked As If It Were Transplanted Due To The Expression Of A Foreign Non-Self Protein On Cell Surfaces

This is by far my most important post. It is also my most disturbing. Yet, it is my greatest hope that it will guide us towards finding solutions.
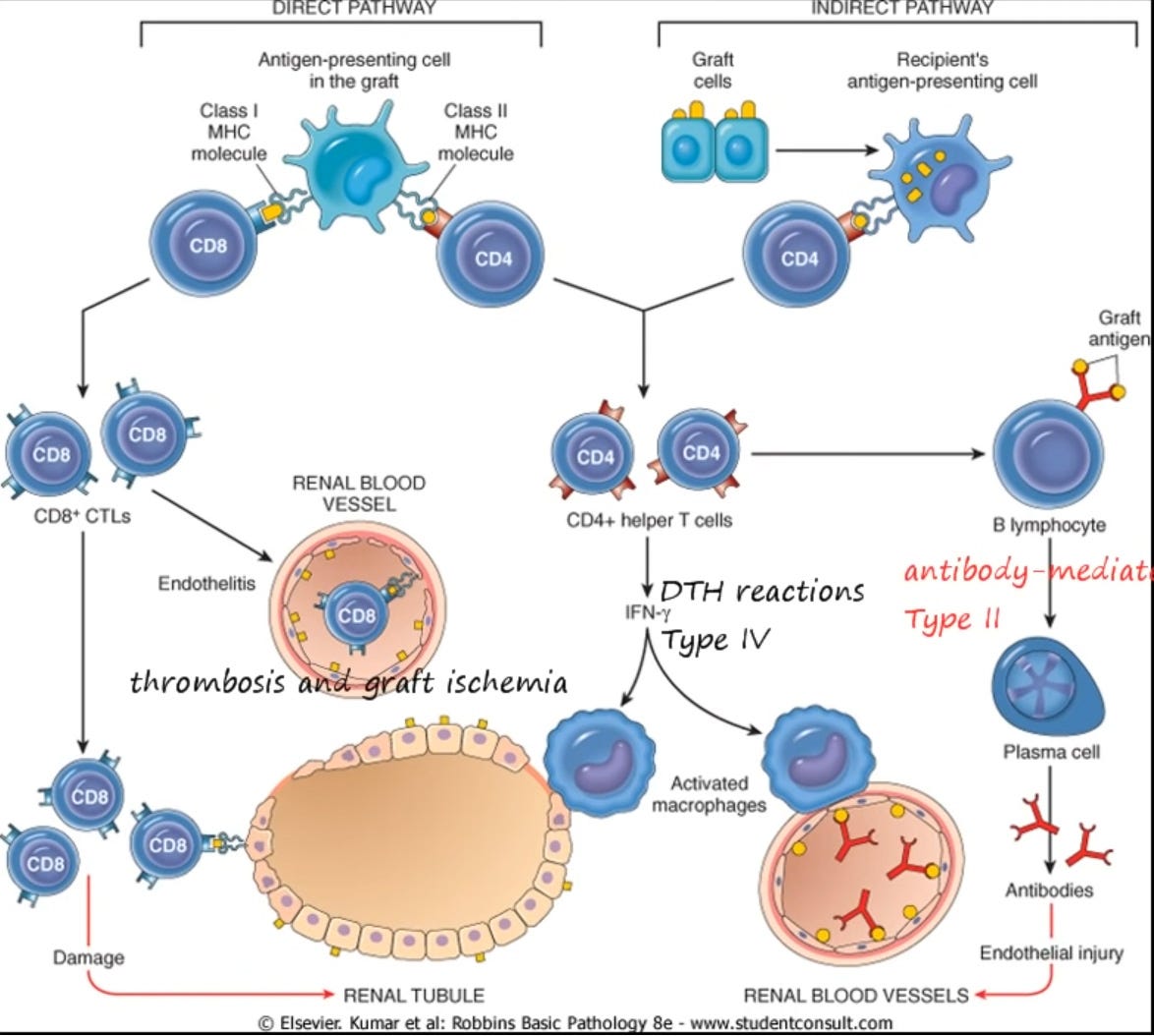
Please study the above image carefully. This is a graphic which shows how the body rejects transplants. Every single individual that receives a transplanted organ will have some level of this type of rejection. The ONLY exception will be if the organ donor happens to be an identical twin of the recipient.
Why? Because identical twins have the same DNA. And there’s the rub. People who are not identical twins of each other have different MHC molecules expressed on their cell surfaces. Virtually every cell in the body has some type of MHC molecule expressed on its surface.
As you can observe, the body identifies the MHC molecule expressed on the transplanted organ is recognized as foreign by the recipient’s immune system and the immune system then begins to attack the organ.
Why is this so extremely dangerous, in the context of the Spike Protein?
REPLACE THE MHC MOLECULE WITH THE SPIKE PROTEIN. Instead of all the cells having a foreign MHC complexes on them, they have SPIKE PROTEINS!
Let us review the symptoms of transplant rejection with each organ, bear in mind Acute/Long COVID and Spike Protein Disease symptoms:
HEART
Patients most commonly present with orthopnea, shortness of breath, paroxysmal nocturnal dyspnea, syncope, palpitations, nausea/loss of appetite, weight gain, edema, arrhythmias (atrial flutter), oliguria, and hypotension. The physical exam can reveal signs of heart failure such as elevated jugular venous pressure, extra sounds on auscultation and peripheral edema.
Heart Transplantation Rejection
https://www.ncbi.nlm.nih.gov/books/NBK537057/
PANCREAS
Given the possibility of chronic rejection, type 1 diabetes mellitus recurrence (in our case, de novo appearance) should also be suspected, which is an infrequent entity, appearing approximately in 3%-7% of properly immunosuppressed patients. It occurs due to the presence of antibodies against pancreatic beta cells in the recipient (type 1 diabetes-associated autoantibodies to the autoantigens GAD65, IA-2, and ZnT8) causing destruction of the pancreatic islets (insulitis). Usually the antibody conversion precede hyperglycemia by a variable length of time, and negative autoimmunity prior to transplantation does not ensure that autoimmune diabetes will not recur.
Late complications of pancreas transplant
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7769730/
LIVER
Rejection is suspected when the liver starts to work less well. This is usually first picked up on blood tests. Occasionally, patients notice that they are jaundiced (yellow).
Rejection of a transplanted liver
https://www.nhsbt.nhs.uk/organ-transplantation/liver/benefits-and-risks-of-a-liver-transplant/risks-of-a-liver-transplant/rejection-of-a-transplanted-liver/
KIDNEY
Many people have no signs or symptoms of kidney rejection. Every person is different. Signs and symptoms of kidney rejection may include:
Feeling like you have the flu, such as body aches, chills, headache and feeling sick to your stomach
Fever of 101° F or higher
Urinating (peeing) less than usual
Having very high blood pressure
Suddenly gaining weight
Swelling in your ankles
Pain or tenderness in your side or belly area
Feeling very tired
Kidney rejection after transplant
https://www.kidneyfund.org/kidney-donation-and-transplant/life-after-transplant-rejection-prevention-and-healthy-tips/kidney-rejection-after-transplant
Clearly, we cannot show Brain Transplant rejection, yet you understand how the symptoms, if it were possible, would be similar. We can look at autoimmune brain diseases. MS, Transverse Myelitis, Neuromyelitis Optica, you get the idea.
How do we know this is possible?
Overall, our results show that the SARS-CoV-2 Spike is abundantly expressed at the surface of infected human pAECs.
SARS-CoV-2 Spike Expression at the Surface of Infected Primary Human Airway Epithelial Cells
https://www.mdpi.com/1999-4915/14/1/5
If we were to look at other cell lines, I am quite certain we would find similar results, because...
Our study demonstrates higher S-protein expression levels in cells treated with Spikevax compared with Comirnaty following an in vitro test. Interestingly, both vaccines showed detectable levels of the S-protein (or truncated forms of it) in the culture media.
Differences in the Expression Levels of SARS-CoV-2 Spike Protein in Cells Treated with mRNA-Based COVID-19 Vaccines: A Study on Vaccines from the Real World
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10144021/
I will continue to work on solutions. At first thought, clearing the Spike is obviously paramount. We must determine how long it is expressed for after infection and vaccination. In either case, let’s hope and pray it is not retrotranscribing.
We have a problem, Houston.
This was my concern from the beginning of the jabs. These jabs are going to trick MY OWN CELLS into creating trillions of foreign proteins? My initial reaction was: "These people have lost their minds! The jabs will most certainly cause an increase in auto-immune diseases." That would be the minimum amount of damage the jabs will cause. Now we know that the foreign protein they chose to have our cells create is itself very toxic, killing some jab recipients soon after injection. The ones who survive the onslaught of trillions of self created toxic proteins can now look forward to autoimmune diseases. What a nightmare!
Thank you Walter. Crimes against humanity. Peace.