

A Radiation-Mimicking Disease of Access: The Only Reason We Initially Believed SARS-CoV-2 was a Respiratory Virus is that the Respiratory Tract is the Initial Point of Access
Wherever the virus and its Spike Protein reach, they mimic the DAMAGE OF RADIATION: RADIATION PNEUMONIA

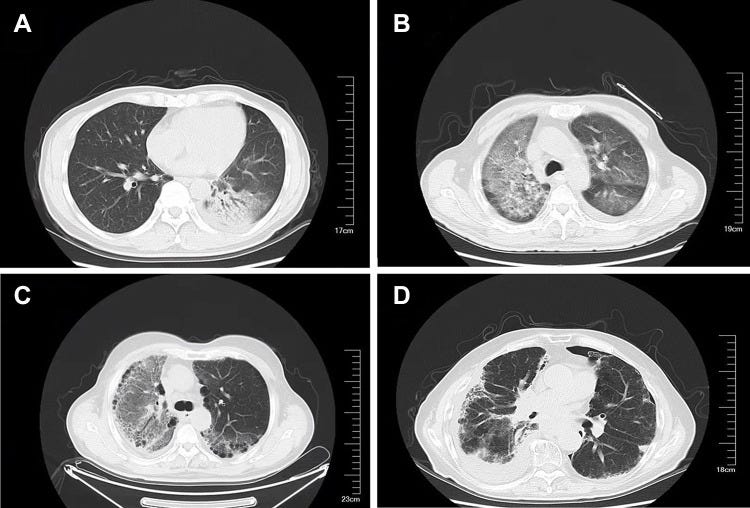
(A) The lower left lung consolidation using an air bronchogram. (B) Ground-glass opacity and mesh opacity of the right lung and the left lung. (C) Ground-glass bilateral lung opacity, with left pleural effusion. (D) Ground-glass opacity, mesh opacity, and pleural effusion of the right lung.
The Spike Protein of SARS-CoV-2 makes its debut (via INFECTION) in the human body through the respiratory tract. Of course, everyone initially believed that this was a respiratory virus causing the deadly pneumonia. However, I believe the evidence is now overwhelming that the pneumonia is caused by the Spike Protein. It does this via a mechanism that precisely mimics Radiation. Please see my previous post for details on this mechanism.
The above graphic is NOT from COVID cases. The graphic is from RADIATION PNEUMONIA cases. In it we see the exact same pathologies we see in COVID pneumonia.
LUNG CONSOLIDATION
Vascular enlargement in consolidative/GGO areas may represent a reasonably common early CT marker in COVID-19 patients and is of uncertain etiology. Although speculative, theoretical mechanisms could potentially reflect acute inflammatory changes, pulmonary endothelial activation, or acute stasis. Further studies are necessary to verify specificity and to study if prognostic for clinical outcomes.
Remarkable vessel enlargement within lung consolidation in COVID-19 compared to AH1N1 pneumonia: A retrospective study in Italy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8135228/
Note how the authors of the above paper claimed the consolidation was of an “uncertain etiology.” We may now say the etiology is certain.
MESH OPACITY
According to a study from Bai et al., compared with non-COVID-19 pneumonia, COVID-19 was more likely to result in peripheral distribution, ground-glass-like shadows, fine-mesh opacity, vascular thickening, and anti-halo signs, which is clearly valuable for differential diagnosis.
Differentiating pneumonia with and without COVID-19 using chest CT images: from qualitative to quantitative
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7505000/
GROUND GLASS OPACITY AND CONSOLIDATION
Seventy-two articles were reviewed for potential inclusion, including 50 discussing chest CT, 15 discussing chest X-ray, five discussing lung ultrasound, and two discussing COVID-19 epidemiology. The reported sensitivities and specificities for chest CT ranged from 64 to 98% and 25 to 88%, respectively. The reported sensitivities and specificities for chest X-rays ranged from 33 to 89% and 11.1 to 88.9%, respectively. The reported sensitivities and specificities for lung ultrasound ranged from 93 to 96.8% and 21.3 to 95%, respectively. The most common findings on chest CT include ground glass opacities and consolidation.
A Review of Crucial Radiological Investigations in the Management of COVID-19 Cases
https://www.cureus.com/articles/142071-a-review-of-crucial-radiological-investigations-in-the-management-of-covid-19-cases#!/
Interestingly, approaching COVID Pneumonia as a mimic of Radiation Pneumonia can also explain the secondary bacterial infections.
Although RP is an aseptic inflammatory disease, patients with severe RP are prone to lung co-infection. A review of relevant literature failed to find a reports pathogenic RP bacteria. In the present study, sputum and/or alveolar lavage fluid were obtained from all patients for culturing. The results showed 25 microorganism cases as well as 9/21 cases of microorganisms with tracheoscopy among the 34 sputum specimens.
And, of course, aggressive antibiotics should have been used in all COVID pneumonia cases.
The use of methylprednisolone is an effective in-patient treatment. Based on the results of the present study, aggressive antibiotic therapy and mechanical ventilation in addition to methylprednisolone administration could reduce patient mortality.
Individual radiosensitivity may be a factor in who experiences severe pneumonia with COVID. The statistics are very similar to Radiation Pneumonia (RP).
Radiotherapy is an important treatment method for lung cancer and other thoracic tumors. Radiation pneumonia (RP) is a common complication of this treatment, with an incidence rate of 5–15% in China. Patients with mild cases of RP who undergo timely treatment have a good prognosis; however, 5–11.7% of patients who develop RP have severe cases of the disease (ie, the patients have a high mortality and are prone to developing pulmonary fibrosis, which affects radiotherapy implementation and can seriously threaten their safety). Radiotherapy, administered either alone or in combination with chemotherapy, helps control tumor growth and prolong patient survival. However, the use of radiotherapy in the treatment of lung cancer and lung metastases can cause injury to healthy lung tissue while killing the tumor.
Clinical Analysis of Severe Radiation Pneumonia
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8216199/
Of note, as stated above, severe RP patients are prone to developing pulmonary fibrosis.
I will continue investigating SARS-CoV-2 and its Spike Protein and how the Spike Protein looks more and more like a “transmissible radiation weapon” - without, of course, using actual radiation.
Hi Walter, early 2021 I found papers showing that Sars-cov-2 had similarities with radiation sickness. My daughter had just been in the ICU with MIS-C and nothing they were telling me added up. I remember hearing a podcast where doctors (I think maybe Dr. Kory Pierre) were saying that the lung disease couldn’t be regular pneumonia because it was showing up in both lungs at once - acute respiratory distress syndrome ARDS. Anyway, the fact that some of these kids were experiencing peeling skin, etc, the whole thing seemed a lot more like a poisoning than a virus. Regardless if your finding pertain to MIS-C or not, thank you for exploring this topic. One question though - even though the spike may cause this radiation type damage, how do you rule out the EMF/5g causing it? I have papers from Dr. Martin Pall that explain how 5g can cause the same type of radiation as ionizing exposure, even though they aren’t the same.
I think that you are right about the spike causing it, but it bothers me that 5g was rolled out at the same time and no one seems to look into it much.
Again, not one of the ppl in the camp of denying the virus, it is way to well documented on all the harms it can cause. But wondered if you think about the environmental factor as well and how they could perhaps both be triggering these symptoms synergistically?
And this was out about a month ago. In the reference to e-coli there was a study that found the shots were not sterile and had e-coli contamination.
"During the interview, McKernan said:
“It’s in both Moderna and Pfizer. We looked at the bivalent vaccines for both Moderna and Pfizer and only the monovalent vaccines for Pfizer because we didn’t have access to monovalent vaccines for Moderna. In all three cases, the vaccines contain double-stranded DNA contamination. If you sequence that DNA, you’ll find that it matches what looks to be an expression vector that’s used to make the RNA…
“Whenever we see DNA contamination, like from plasmids, ending up in any injectable, the first thing people think about is whether there’s any E. coli endotoxin present because that creates anaphylaxis for the injected. And, of course, your viewers and listeners are probably aware there’s a lot of anaphylaxis going on, not only on TV but in the VAERS database. You can see people get injected with this and drop. That could be the background from this E. coli process of manufacturing the DNA…"