

A Lining Cell Disease - Beyond the Endothelium: The Spike Protein Induces Inflammation and Destruction of Organ and Cell Linings
The Spike Protein of SARS-CoV-2 attacks the lining of virtually every major organ and system inducing chronic inflammation and destruction.

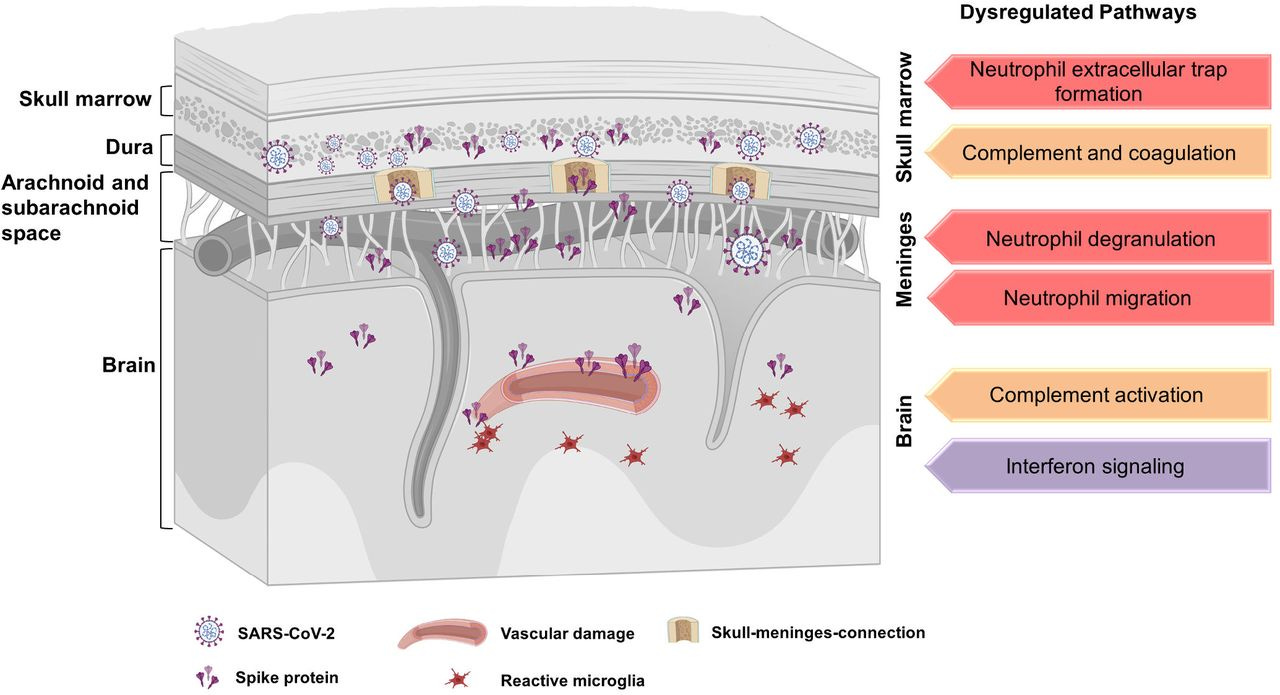
Short Summary The accumulation of SARS-CoV-2 spike protein in the skull-meninges-brain axis presents potential molecular mechanisms and therapeutic targets for neurological complications in long-COVID-19 patients.
Readers of this Substack and my X account have long known that I have called the Endothelial dysfunction (and its consequences) caused by the Spike Protein SPED (Spike Protein Endothelial Disease). However, given the immense systemic complications caused by the Spike Protein, I eventually found this to be an insufficient explanation for what is being observed.
I have now arrived at a broader understanding of the Spike Protein. It is not a question of a Blood Vessel disease alone – although it is, indeed that, too. The Spike Protein is far more versatile. It has the ability to invade virtually every organ and cell lining in the body. Not just the Endothelium. The Epithelium, the Pericardium, the Meninges, the Liver Sinusoids. A massive, fibrotic, sclerotic assault on the major functions of the body. And it is slow. And the band plays on.
LIVER SINUSOIDS
Steatosis, single-cell and focal/zonal hepatocyte necrosis, portal fibrosis, and chronic inflammation were found in varying percentages. Sinusoidal ectasia, endothelial cell disruption, and fibrin-filled sinusoids were seen in all cases; these were assessed semiquantitatively for severity (SEF scored). SEF scores did not correlate with cause-of-death categories (p = 0.92) or with severity of lung alterations (p = 0.96). SARS-CoV-2 RNA was detected in 13/20 cases by PCR and in 9/20 by ISH, with IHC demonstration of spike protein in 4/20 cases and NP in 15/20.
Liver alterations and detection of SARS-CoV-2 RNA and proteins in COVID-19 autopsies
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9759055/
BRAIN MENINGES
Our results revealed the accumulation of the spike protein in the skull marrow, brain meninges, and brain parenchyma. The injection of the spike protein alone caused cell death in the brain, highlighting a direct effect on brain tissue. Furthermore, we observed the presence of spike protein in the skull of deceased long after their COVID-19 infection, suggesting that the spike’s persistence may contribute to long-term neurological symptoms. The spike protein was associated with neutrophil-related pathways and dysregulation of the proteins involved in the PI3K-AKT as well as complement and coagulation pathway. Overall, our findings suggest that SARS-CoV-2 spike protein trafficking from CNS borders into the brain parenchyma and identified differentially regulated pathways may present insights into mechanisms underlying immediate and long-term consequences of SARS-CoV-2 and present diagnostic and therapeutic opportunities.
SARS-CoV-2 Spike Protein Accumulation in the Skull-Meninges-Brain Axis: Potential Implications for Long-Term Neurological Complications in post-COVID-19
https://www.biorxiv.org/content/10.1101/2023.04.04.535604v1.full
HEART PERICARDIUM
In this study, inflammatory foci were predominantly in the right heart, suggesting a gradual bloodstream-derived exposure, which raises speculation that an inadvertently large dose of the vaccination with IV injection may contribute to development of myocarditis. Immunostaining reflected presence of SARS-CoV-2 spike–RBD protein in cardiomyocytes, infiltrating immune cells and vascular endothelial cells within the myocardium and pericardium.
Shedding Light on Mechanisms of Myocarditis With COVID-19 mRNA Vaccines
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10010664/
GI TRACT
To systemically characterize intestinal infection and inflammation in COVID‐19 patients, we evaluated different segments of intestinal tissues from 18 patients who were diagnosed with COVID‐19 and presented with GI symptoms (Table EV1). Robust expression of virus receptor ACE2 and virus antigen spike protein was detected in small intestine (Fig EV1A and B), indicating SARS‐CoV‐2 infection in GI tract, which agreed with previous studies (Du et al, 2020; Zhang et al, 2020). Intriguingly, small intestine displayed the most severe inflammation characterized by inflammatory cell infiltration and signs of vascular damage such as interstitial edema, hemorrhage and vasodilation.
SARS‐CoV‐2 spike spurs intestinal inflammation via VEGF production in enterocytes
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9081906/
MYELIN (LINING OF NERVE CELLS)
In addition to loss of taste and smell, inflammatory demyelinating polyneuropathy and Guillain-Barré syndrome (GBS) have also been reported in Covid-19 infections. SARS-CoV-2 seems to have neurotropism and can trigger demyelination by directly injuring myelin- producing cells or causing inflammation.
SARS-CoV-2 entry sites are present in all structural elements of the human glossopharyngeal and vagal nerves: Clinical implications
https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(22)00165-7/fulltext
In essence, the Endothelium is simply a gateway. The Spike Protein invades organs – from the outside in, ironically slowly killing from the inside out. And this really isn’t a surprise. After all, ACE2 is literally the absolute most dangerous receptor if you wanted to design something to attack the human body. It is everywhere.
The more we learn, the better strategies and treatments we can determine to keep the Spike Protein at bay. COVID and Long COVID are diseases of access. Deny the Spike Protein entry, game over for SARS-CoV-2. The question of viral persistence is still of concern, as it retrotranscription.
It may be that for a certain percentage of the population lifelong therapy will be needed to keep Spike levels low. The same as HIV patients need lifelong therapy to keep HIV levels low.
Thank you for your readership, dialog and support. I will continue to study and report in our battle against this unnatural virus and its proteins.
I have chronic/ systemic inflammatory response syndrome. From biotoxin mold illness. And other autoimmune. I’m seeing so many people, seems like they have the same problem now. & whatever “ shedding “ is, is a constant challenge now.
So how can one who is mRNA vaxed measure the amounts of spike proteins in his system, if any? Is the most common indicator of the presence of spikes seeing microclotting as shown on a d-dimer test? Or could one have spikes proteins present without microclotting and with a normal d-dimer test result?