
HAAV: Human Accelerated Aging Virus: Refining My SARS-CoV-2 Accelerated Aging Hypothesis
HAAV: Human Accelerated Aging Virus: Refining My SARS-CoV-2 Accelerated Aging Hypothesis
SARS-CoV-2 is a serious infection. In a parallel to FIP, an innocuous initial infection may seed a long-term fatal disease.

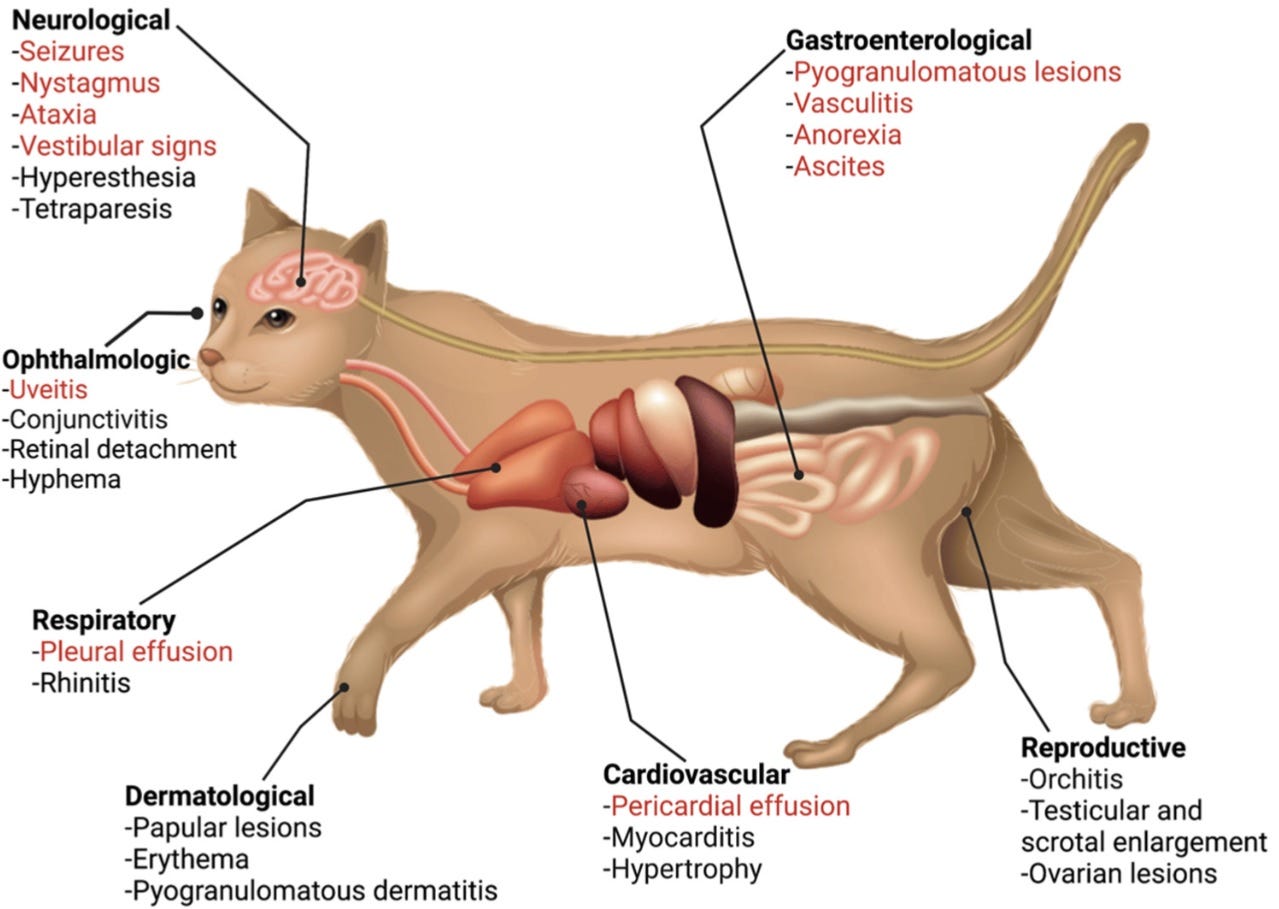
Summary of the systemic clinical signs and pathologies associated with FIP. FIP is well known to be a systemic infection with a diverse presentation. The possible systemic clinical signs associated with FIP, encompassing the organ systems that are also affected by COVID-19, are summarized. The most common signs of FIP are colored in red.
Clinical and Molecular Relationships between COVID-19 and Feline Infectious Peritonitis (FIP)
https://www.mdpi.com/1999-4915/14/3/481
As readers of this Substack know, I have, from the beginning, been concerned about how SARS-CoV-2 appears to accelerate aging in those infected. Numerous studies have borne this out. However, I now propose a mechanism which can explain, in broader terms, how this accelerated aging may occur – and it is related to how FCoV causes the fatal FIP.
First, it is important to understand that cats which develop FIP may have low, undetectable or non-existent levels of antibodies.
Opinions on the value of antibody measurement for the diagnosis of FIP vary, but based on the results of numerous studies, which are shown in the following paragraphs, it is the authors’ opinion that antibody measurement is of no use in a cat suspected of having FIP. If antibodies are measured in a cat suspected of having FIP, then a titer should be determined in any case. Especially low and medium titers are of zero diagnostic value for the diagnosis of FIP [16,78]. Although a rising titer can sometimes be detected during progression of the disease [55,60], this can also be seen in conjunction with FECV reinfection, and thus is not an indicator for FIP [70]. High and rising titers can also be found in healthy FECV-infected cats [70,73] and should never be used to confirm a suspicion of FIP. Likewise, a negative antibody test result cannot exclude FIP [79,80]. In end-stage FIP, especially with fulminant effusions, declining antibody titers are possible and sometimes antibody concentrations can even drop below the limit of detection [60,68]. Approximately 10% of cats with FIP do not have serum antibodies.
Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6893704/
Furthermore, an FCoV infection which leads to FIP may initially be so mild as to be of no mention or present no obvious symptoms at all.
Cats that have been initially exposed to FeCV usually show no obvious symptoms. Some cats may show mild upper respiratory symptoms such as sneezing, watery eyes, and nasal discharge, while others may experience mild gastrointestinal signs such as diarrhea. In most cases, these mild signs are self-limiting.
Feline Infectious Peritonitis
https://www.vet.cornell.edu/departments-centers-and-institutes/cornell-feline-health-center/health-information/feline-health-topics/feline-infectious-peritonitis
Now, let’s discuss how an FCoV infection becomes FIP.
In approximately 10 percent of cats infected with FeCV, one or more mutations of the virus can alter its biological behavior, resulting in white blood cells becoming infected with virus and spreading it throughout the cat’s body. When this occurs, the virus is referred to as the FIPV. An intense inflammatory reaction to FIPV occurs around vessels in the tissues where these infected cells locate, often in the abdomen, kidney, or brain. It is this interaction between the body’s own immune system and the virus that is responsible for the development of FIP.
Feline Infectious Peritonitis
https://www.vet.cornell.edu/departments-centers-and-institutes/cornell-feline-health-center/health-information/feline-health-topics/feline-infectious-peritonitis
However, with the Spike Protein of SARS-CoV-2, we have a ready-made mechanism that needs no mutation to effect this spread, inducing those inflammatory reactions! That is, ultimately, Spike Protein Endothelial Disease (SPED). This allows the Spike Protein to spread throughout the body.
The way in which SARS-CoV-2 induces HAAV I propose is quite different from the mechanism by which FIP kills. In HAAV, I propose that the Spike Protein (almost certainly produced by reservoirs and/or mRNA) continues to elicit almost imperceptible low levels of chronic inflammation.
In this cross-sectional study, blood samples were obtained from three different sites in Australia from individuals with i) a resolved SARS-CoV-2 infection (and no persistent symptoms i.e. Recovered), ii) individuals with prolonged PASC-CVS and iii) SARS-CoV-2 negative individuals. Individuals with PASC-CVS, relative to Recovered individuals, had a blood transcriptomic signature associated with inflammation. This was accompanied by elevated levels of pro-inflammatory cytokines (IL-12, IL-1beta;, MCP-1 and IL-6) at approximately 18 months post-infection. These cytokines were present in trace amounts, such that they could only be detected with the use of novel nanotechnology. Importantly, these trace-level cytokines had a direct effect on the functionality of pluripotent stem cell derived cardiomyocytes in vitro.
Cardiovascular symptoms of PASC are associated with trace-level cytokines that affect the function of human pluripotent stem cell derived cardiomyocytes
https://www.biorxiv.org/content/10.1101/2024.04.11.587623v1
This can explain virtually all of the diseases of aging we see emerging in ever younger populations.
Clearly, it concerns me when I hear that COVID is a “nothing burger.” Obviously, more study is needed to determine the levels to which this may be occurring. Perhaps it is best to keep in mind that HIV also follows a similar route – an initially “nothing burger” “cold.”
I will continue to research this finding. As we learn more, finding the truth becomes ever more possible. Thank you for your continued support, readership and dialog.
Walter ….. it has come to light that the COVID virus as known currently was NOT isolated ( identified) in the lab at Wuhan where it originated. As with every virus certain protocols are used to properly identify a virus. This was not done apparently and recently admitted to by one of the leading scientists working there. Not that this matters per se with the virus as it seems the spike is the big cause of the problems. However with the genetic sequence of the virus ( now questionable ) being handed to Ralph Baric at UNC and also EcoHealth and presumably the vaccine manufacturers, would this account for how useless the shots have performed and being non neutralizing they would allow a far larger breeding ground for variants?
Another tour de force. We must not let hysteria overwhelm us, and be guided by the facts, wherever they may lead.
It always seemed obvious from the start that a vaccine that only works by converting your cells into antigen producers was misconceived folly disguised as genius, as was a mass vaccination program in the middle of a pandemic.
My mother was born before vaccines and penicillin, and never had a serious disease all her life, and lived through two world wars, a Great Depression and two pandemics, eating only home cooked foods, fresh water and walking half a mile each day. She only took one low dose aspirin each day, which I take as well and she had a Noah’s Arc microbiome as a shield against any infection.
Public health, clean water, toilets in each house, fortified foods, were here long before vaccines, a fact that is always ignored by health experts who like to rewrite history of disease eradication.