

For the First Time, A Peer Reviewed Paper Supports My Hypothesis Held from the Beginning: Infection and Transfection Both Contributing to Sudden Cardiac Deaths
McGonagle and Giryes demonstrate how induced chronic inflammation in the vasa vasorum may be the driving factor. Spike is Spike.

Potential Links between coronary artery disease and COVID-19 era excess mortality seemingly unlinked to viral infection.
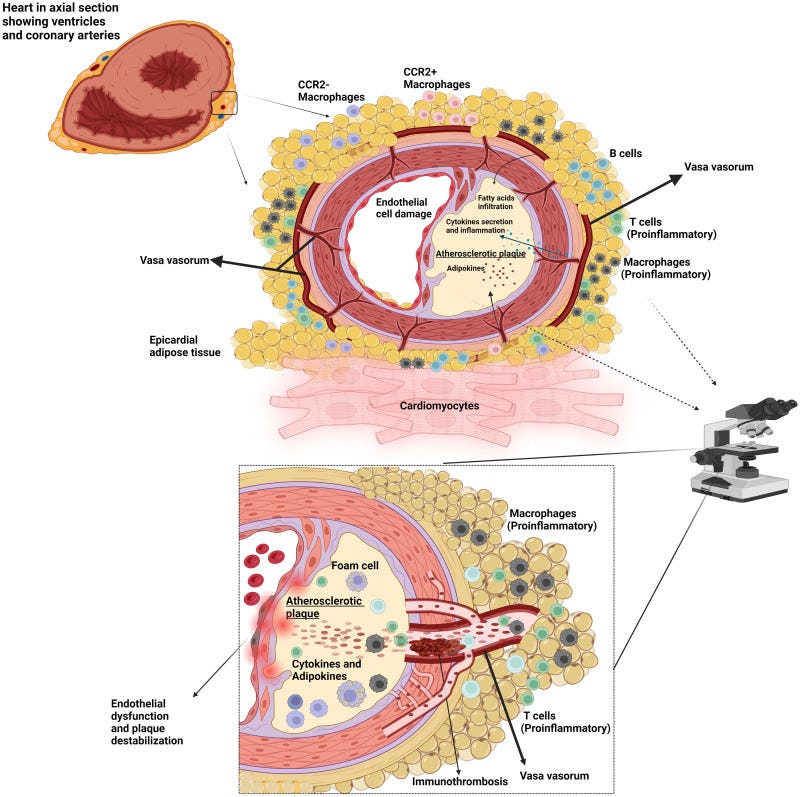
Diagram showing the complexity of the biomechanical and immunological environment of the proximal coronary arteries in the epicardial fat. Given the propensity of isolated coronary artery disease to occur at this site rather than more distally, it likely represents one of the most key immune territories in late complications not ostensibly linked to viral disease. A key unresolved area is the link between coronary artery intimal disease and to what extent it depends on the epicardial vasa vasorum function or whether a direct impact of viral infection or viral constituent nucleic acid or proteins directly dysregulate the artery intima.
I would like to begin this post with a statement from the conclusion of the paper we will be discussing:
For the first time in the history of immunology the immune system has simultaneously faced an attack from without (natural infection) and near simultaneously vaccine mediated immune activation from within. Unfortunately, much evidence points towards inflammation in the vicinity of “widow-maker” coronary artery territories for several microbes and even vaccines. With particular respect to coronavirus is the potential impact of spike protein itself on coronary artery and cardiovascular biology that is a further potentially relevant factor [118].
The perception that there is a fear of investigating the current excess deaths is probably driven by a reticence towards uncovering a negative link with coronavirus vaccinations that might be perceived to undermine general societal confidence or the public health drive to “eradicate the virus.”
An immunology model for accelerated coronary atherosclerosis and unexplained sudden death in the COVID-19 era
https://www.sciencedirect.com/science/article/pii/S1568997224001332
There it is. What I have maintained from the beginning. Spike is Spike. However, it seems quite apparent that the volume of Spike endured from transfection is on the orders of magnitude greater than that experienced from natural infection.
What McGonagle and Giryes have shown us in their paper published online for the November issue of Autoimmunity Reviews is that the Spike Protein (clearly, as that is the only viral protein expressed in the transfection) causes chronic inflammation of the vasa vasorum.
For those who may not be familiar with the vasa vasorum, here is a brief summary:
Vasa vasorum are blood microvessels which penetrate the adventitia and outer layers of the media of large blood vessels, supplying them with nutrients and oxygen. A growing body of evidence suggests that vasa vasorum play a central role in the pathogenesis of atherosclerosis. In this review, we will make a case for the role of microvascular dysfunction in the initiation of disease. When seen through this lens, new therapeutic opportunities for prevention can be envisioned. In particular, we discuss how targeting the cellular metabolism and epigenetic machinery of vasa vasorum neovessels could be harnessed to render vasa vasorum endothelial cells less sensitive to atherogenic stimuli.
Targeting vasa vasorum dysfunction to prevent atherosclerosis
https://www.sciencedirect.com/science/article/abs/pii/S1537189117301635
And how this relates to the increase in sudden cardiac deaths is detailed by McGonagle and Giryes further into their paper.
The coronary artery vasa vasorum resides in the visceral pericardium or epicardial tissue that is adipose rich and is physiologically a liquid at body temperature thus contributing to shock absorption and likely contributes to normal coronary arteries homeostasis in adults. The epicardial adipose tissue (EAT) contains several types of immune cells including macrophages and B cells, and these cells play an important role in vascular development, homeostasis and repair, remodelling and immunosurveillance. Cardiac yolk sac derived macrophages (CC chemokine receptor type 2 negative (CCR2-)) populate the heart during embryogenesis and persists throughout life and are essential for the coronary artery maturation. The EAT resident macrophage population is capable of induction of high levels of multiple pro-inflammatory cytokines. One of the unique features of epicardial adipose tissue that is contiguous with the myocardium without muscle facia and share the same microcirculation. In pathological conditions, epicardial adipose tissue can become pro-atherogenic and pro-arrhythmogenic due to increased pro-inflammatory macrophage activity. The arrhythmogenic potential is likely secondary to the loss of fatty insulation immediately adjacent to the sinoatrial and atrioventricular nodes.
Beyond direct triggering of atherosclerotic disease, epicardial tissue disruption of electrochemical homeostasis of the conducting tissue could also predispose to various atrial and ventricular arrhythmia. Accordingly, the presence of a pandemic with a widely circulating virus and potentially the simultaneous boosting of coronavirus immunity provides a credible mechanism for unexplained cardiovascular disease that is not evidently an acute vasculitis pathology, nor immediately evident as an immunologically driven process but rather manifests as a late atherosclerotic sequela.
An immunology model for accelerated coronary atherosclerosis and unexplained sudden death in the COVID-19 era
https://www.sciencedirect.com/science/article/pii/S1568997224001332
So, we have an explanation for both the excess arrhythmic sudden deaths and the excess sudden deaths caused by infarction. This, unfortunately, elegantly ties together all my hypotheses about what the Spike Protein would do. From SPED, to chronic inflammation to systemic microvascular disease of which, clearly, the vaso vasorum is a part.
I take no pleasure in my hypotheses being supported by clinical evidence and potentially being proven true. If there is a silver lining, it is that having already researched therapeutics to ameliorate the predicted pathologies may put us ahead of the curve in successfully treating/preventing Spike Protein injury and disease.
I will continue to work, and, as always, thank you for your support, readership and dialog.
In the beginning the Salk Institute had written an article essentially saying the same thing as "spike is spike". I screenshot that article. The following day the article was changed to a word salad of why 1 spike was better than the other... my spidey sense went off...lol. so grateful I never got the type in the syringe. Thank you for your continued articles. Hyperbaric Oxygen Chambers work for everyone to lower inflammation!
Spike is spike but obviously injecting spike and forcing your body to become a spike factory ... is far far far more dangerous... than contracting covid
THE VACCINES ARE CAUSING THE HEART DAMAGE... NOT COVID